

Who should have surgery for an intervertebral disc herniation? Comparative effectiveness evidence from the spine patient outcomes research trial
- PMID: 21681140
- PMCID: PMC3472961
- DOI: 10.1097/BRS.0b013e3182276b2b
Who should have surgery for an intervertebral disc herniation? Comparative effectiveness evidence from the spine patient outcomes research trial
Abstract
Study design: Combined prospective randomized controlled trial and observational cohort study of intervertebral disc herniation (IDH), an as-treated analysis.
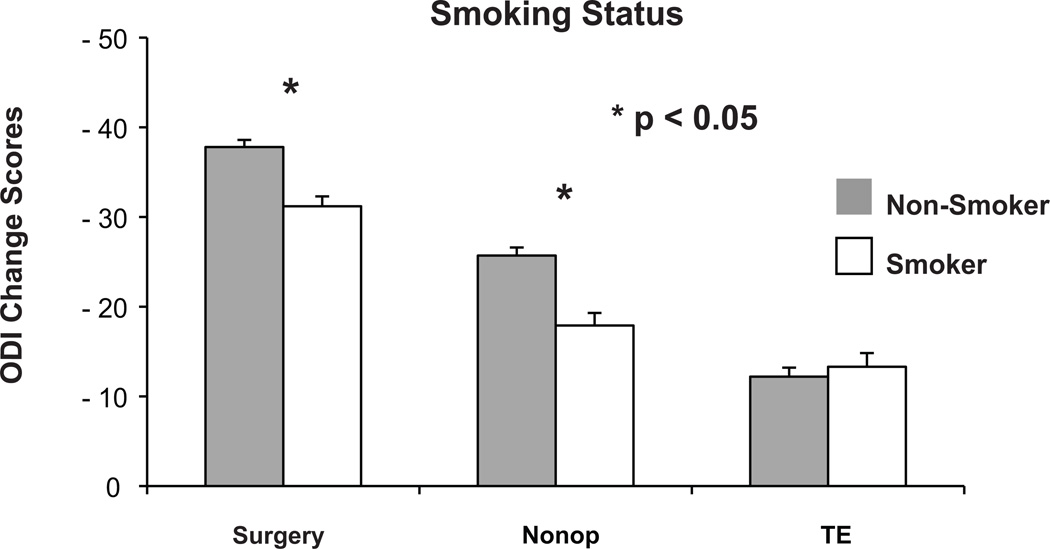
Objective: To determine modifiers of the treatment effect (TE) of surgery (the difference between surgical and nonoperative outcomes) for intervertebral disc herniation (IDH) using subgroup analysis.
Summary of background data: The Spine Patient Outcomes Research Trial demonstrated a positive surgical TE for IDH at the group level. However, individual characteristics may affect TE. No prior studies have evaluated TE modifiers in IDH.
Methods: IDH patients underwent either discectomy (n = 788) or nonoperative care (n = 404) and were analyzed according to treatment received. Thirty-seven baseline variables were used to define subgroups for calculating the time-weighted average TE for the Oswestry Disability Index (ODI) across 4 years (TE = ΔODI(surgery) -ΔODI(nonoperative)). Variables with significant subgroup-by-treatment interactions (P < 0.1) were simultaneously entered into a multivariate model to select independent TE predictors.
Results: All analyzed subgroups improved significantly more with surgery than with nonoperative treatment (P < 0.05). In minimally adjusted univariate analyses, being married, absence of joint problems, worsening symptom trend at baseline, high school education or less, older age, no worker's compensation, longer duration of symptoms, and an SF-36 mental component score (MCS) less than 35 were associated with greater TEs. Multivariate analysis demonstrated that being married (TE, -15.8 vs. -7.7 single, P < 0.001), absence of joint problems (TE, -14.6 vs. -10.3 joint problems, P = 0.012), and worsening symptoms (TE, -15.9 vs. -11.8 stable symptoms, P = 0.032) were independent TE modifiers. TEs were greatest in married patients with worsening symptoms (-18.3) vs. single patients with stable symptoms (-7.8).
Conclusion: IDH patients who met strict inclusion criteria improved more with surgery than with nonoperative treatment, regardless of specific characteristics. However, being married, without joint problems, and worsening symptom trend at baseline were associated with a greater TE.
Figures




References
-
- Abramovitz JN, Neff SR. Lumbar disc surgery: results of the Prospective Lumbar Discectomy Study of the Joint Section on Disorders of the Spine and Peripheral Nerves of the American Association of Neurological Surgeons and the Congress of Neurological Surgeons. Neurosurgery. 1991;29:301–307. discussion 7–8. - PubMed
-
- Astrand P, Maattanen H, Vucetic N, Svensson O. Pain and orthopaedic and neurologic signs after lumbar discectomy: a 2-year followup. Clinical orthopaedics and related research. 2000:154–160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
