

Mutations in the TGFβ binding-protein-like domain 5 of FBN1 are responsible for acromicric and geleophysic dysplasias
- PMID: 21683322
- PMCID: PMC3135800
- DOI: 10.1016/j.ajhg.2011.05.012
Mutations in the TGFβ binding-protein-like domain 5 of FBN1 are responsible for acromicric and geleophysic dysplasias
Abstract
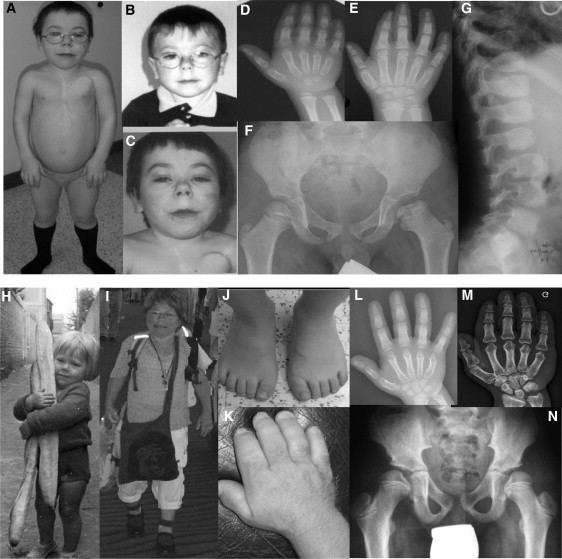
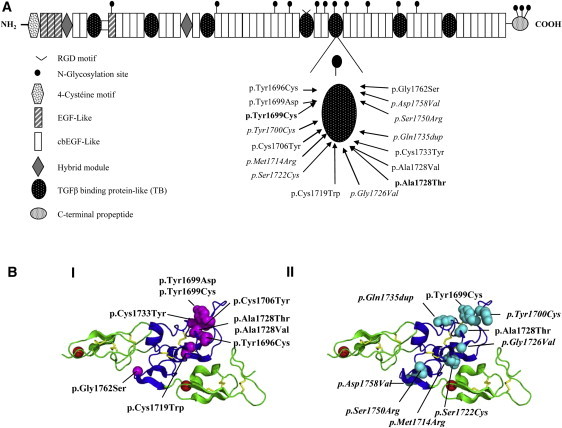
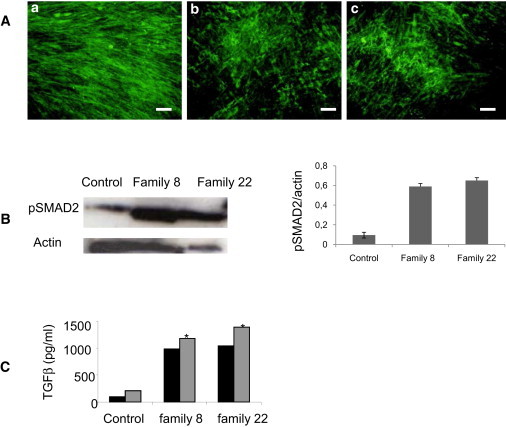
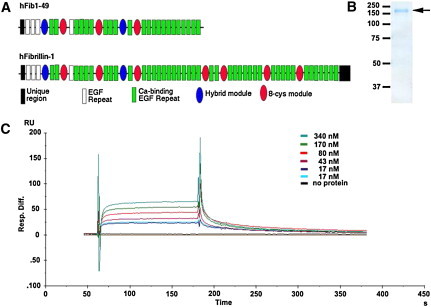
Geleophysic (GD) and acromicric dysplasia (AD) belong to the acromelic dysplasia group and are both characterized by severe short stature, short extremities, and stiff joints. Although AD has an unknown molecular basis, we have previously identified ADAMTSL2 mutations in a subset of GD patients. After exome sequencing in GD and AD cases, we selected fibrillin 1 (FBN1) as a candidate gene, even though mutations in this gene have been described in Marfan syndrome, which is characterized by tall stature and arachnodactyly. We identified 16 heterozygous FBN1 mutations that are all located in exons 41 and 42 and encode TGFβ-binding protein-like domain 5 (TB5) of FBN1 in 29 GD and AD cases. Microfibrillar network disorganization and enhanced TGFβ signaling were consistent features in GD and AD fibroblasts. Importantly, a direct interaction between ADAMTSL2 and FBN1 was demonstrated, suggesting a disruption of this interaction as the underlying mechanism of GD and AD phenotypes. Although enhanced TGFβ signaling caused by FBN1 mutations can trigger either Marfan syndrome or GD and AD, our findings support the fact that TB5 mutations in FBN1 are responsible for short stature phenotypes.
Copyright © 2011 The American Society of Human Genetics. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Spranger J.W., Gilbert E.F., Tuffli G.A., Rossiter F.P., Opitz J.M. Geleophysic dwarfism—a “focal” mucopolysaccharidosis? Lancet. 1971;2:97–98. - PubMed
-
- Maroteaux P., Stanescu R., Stanescu V., Rappaport R. Acromicric dysplasia. Am. J. Med. Genet. 1986;24:447–459. - PubMed
-
- Le Goff C., Morice-Picard F., Dagoneau N., Wang L.W., Perrot C., Crow Y.J., Bauer F., Flori E., Prost-Squarcioni C., Krakow D. ADAMTSL2 mutations in geleophysic dysplasia demonstrate a role for ADAMTS-like proteins in TGF-beta bioavailability regulation. Nat. Genet. 2008;40:1119–1123. - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
