

Who is the high-risk recipient? Predicting mortality after heart transplant using pretransplant donor and recipient risk factors
- PMID: 21683337
- PMCID: PMC4243707
- DOI: 10.1016/j.athoracsur.2011.02.086
Who is the high-risk recipient? Predicting mortality after heart transplant using pretransplant donor and recipient risk factors
Abstract
Background: In this study we sought the following: (1) To objectively assess the risk related to various pretransplant recipient and donor characteristics; (2) to devise a preoperative risk stratification score (RSS) based on pretransplant recipient and donor characteristics predicting graft loss at 1 year; and (3) to define different risk strata based on RSS.
Methods: The United Network for Organ Sharing provided de-identified patient-level data. Analysis included 11,703 orthotopic heart transplant recipients aged 18 years or greater and transplanted between January 1, 2001 and December 31, 2007. The primary outcome was 1-year graft failure. Multivariable logistic regression analysis (backward p value<0.20) was used to determine the relationship between pretransplant characteristics and 1-year graft failure. Using the odds ratio for each identified variable, an RSS was devised. The RSS strata were defined by calculating receiver operating characteristic curves and stratum specific likelihood ratios.
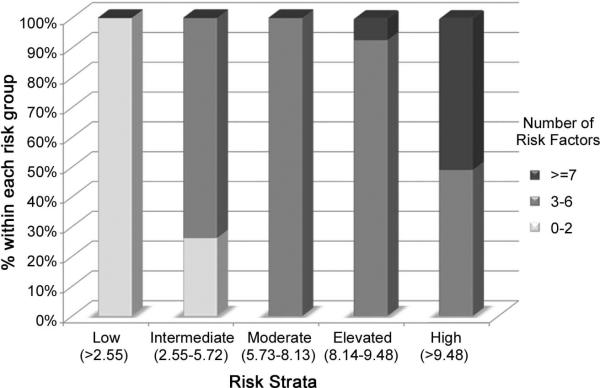
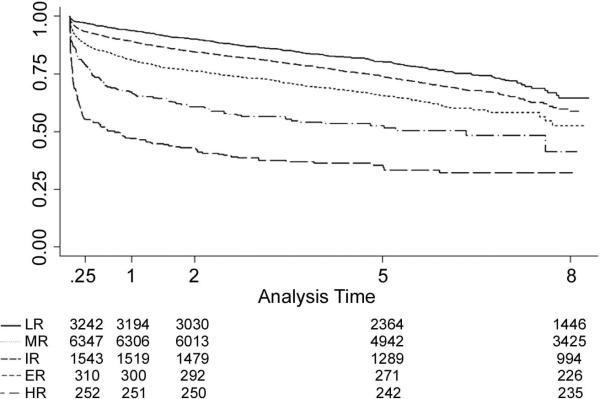
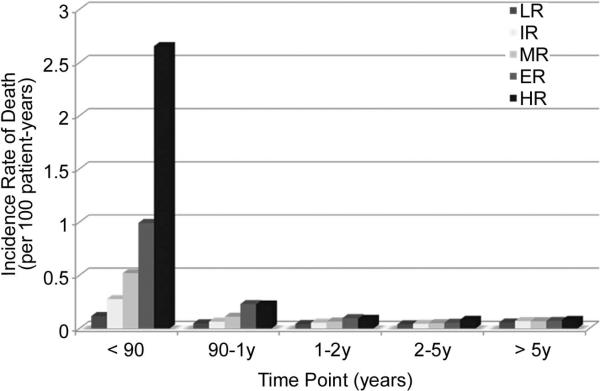
Results: The strongest negative predictors of 1-year graft failure included the following: right ventricular assist device only, extracorporeal membrane oxygenation, renal failure, extracorporeal left ventricular assist device, total artificial heart, and advanced age. Threshold analysis identified 5 discrete RSS strata: low risk (LR, RSS: <2.55; n=3242, 27.7%), intermediate risk (IR, RSS: 2.55-5.72; n=6,347, 54.2%), moderate risk (MR, RSS: 5.73-8.13; n=1,543, 13.2%), elevated risk (ER, RSS: 8.14-9.48; n=310, 2.6%), and high risk (HR, RSS: >9.48; n=261, 2.2%). The 1-year actuarial survival (%) in the LR, IR, MR, ER, and HR groups were 93.8, 89.2, 81.3, 67.0, and 47.0, respectively.
Conclusions: Pretransplant recipient variables significantly influence early and late graft failure after heart transplantation. The RSS may improve organ allocation strategies by reducing the potential negative impact of transplanting candidates who are at a high risk for poor postoperative outcomes.
Copyright © 2011 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Russo MJ, Chen JM, Hong KN, et al. Survival After Heart Transplantation Is Not Diminished Among Recipients With Uncomplicated Diabetes Mellitus: An Analysis of the United Network of Organ Sharing Database. Circulation. 2006;114:2280–2287. - PubMed
-
- Luckraz H, Sharples LD, Charman SC, et al. Does Heart Transplantation Confer Survival Benefit in All Risk Groups? J Heart Lung Transplant. 2005;24:1231–1234. - PubMed
-
- Russo MJ, Chen JM, Sorabella RA, et al. The effect of ischemic time on survival after heart transplantation varies by donor age: An analysis of the United Network of Organ Sharing Database. J Thorac Cardiovasc Surg. 2007;133:554–559. - PubMed
-
- OPTN/DRTR [January 27, 2010];Annual Report. 2008 Available at http://www.ustransplant.org/annual_reports/current/313_ord.htm.
-
- Zaroff JG, Rosengard BR, Armstrong WF, et al. Consensus conference report: maximizing use of organs recovered from the cadaver donor: cardiac recommendations, March 28-29, 2001, Crystal City, Va. Circulation. 2002;106:836–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
