

Diabetes is not associated with increased mortality in emergency department patients with sepsis
- PMID: 21683473
- PMCID: PMC3425373
- DOI: 10.1016/j.annemergmed.2011.03.052
Diabetes is not associated with increased mortality in emergency department patients with sepsis
Abstract
Study objective: Despite its high prevalence, the influence of diabetes on outcomes of emergency department (ED) patients with sepsis remains undefined. Our aim is to investigate the association of diabetes and initial glucose level with mortality in patients with suspected infection from the ED.
Methods: Three independent, observational, prospective cohorts from 2 large US tertiary care centers were studied. We included patients admitted to the hospital from the ED with suspected infection. We investigated the association of diabetes and inhospital mortality within each cohort separately and then overall with logistic regression and generalized estimating equations adjusted for age, sex, disease severity, and sepsis syndrome. We also tested for an interaction between diabetes and hyperglycemia/hypoglycemia.
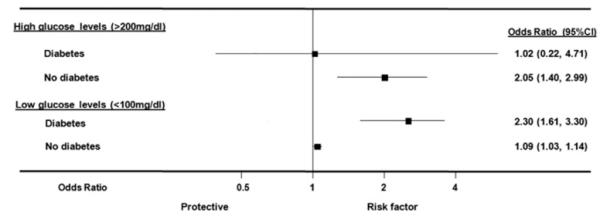
Results: A total of 7,754 patients were included. The mortality rate was 4.3% (95% confidence interval [CI] 3.9% to 4.8%) and similar in diabetic and nondiabetic patients (4.1% versus 4.4%; absolute risk difference 0.4%; 95% CI -0.7% to 1.4%). There was no significant association between diabetes and mortality in adjusted analysis (odds ratio [OR] overall 0.85; 95% CI 0.71 to 1.01). Diabetes significantly modified the effect of hyperglycemia and hypoglycemia with mortality; initial glucose levels greater than 200 mg/dL were associated with higher mortality in nondiabetic patients (OR 2.1; 95% CI 1.4 to 3.0) but not in diabetic patients (OR 1.0; 95% CI 0.2 to 4.7), whereas glucose levels less than 100 mg/dL were associated with higher mortality mainly in the diabetic population (OR 2.3; 95% CI 1.6 to 3.3) and to a lesser extent in nondiabetic patients (OR 1.1; 95% CI 1.03 to 1.14).
Conclusion: We found no evidence for a harmful association of diabetes and mortality in patients across different sepsis severities. High initial glucose levels were associated with adverse outcomes in the nondiabetic population only. Further investigation is warranted to determine the mechanism for these effects.
Copyright © 2011 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Figures


References
-
- Stegenga ME, Vincent JL, Vail GM, et al. Diabetes does not alter mortality or hemostatic and inflammatory responses in patients with severe sepsis. Crit Care Med. 2010;38:539–545. - PubMed
-
- Bernard GR. Drotrecogin alfa (activated) (recombinant human activated protein C) for the treatment of severe sepsis. Crit Care Med. 2003;31(1 suppl):S85–93. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–1377. - PubMed
-
- Shapiro N, Howell MD, Bates DW, et al. The association of sepsis syndrome and organ dysfunction with mortality in emergency department patients with suspected infection. Ann Emerg Med. 2006;48:583–590. e581. - PubMed
-
- Shapiro NI, Howell MD, Talmor D, et al. Mortality in Emergency Department Sepsis (MEDS) score predicts 1-year mortality. Crit Care Med. 2007;35:192–198. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
