

The impact of disease distribution on survival in patients with stage III epithelial ovarian cancer cytoreduced to microscopic residual: a Gynecologic Oncology Group study
- PMID: 21683993
- PMCID: PMC3670691
- DOI: 10.1016/j.ygyno.2011.04.041
The impact of disease distribution on survival in patients with stage III epithelial ovarian cancer cytoreduced to microscopic residual: a Gynecologic Oncology Group study
Abstract
Objective: To assess the survival impact of initial disease distribution on patients with stage III epithelial ovarian cancer (EOC) cytoreduced to microscopic residual.
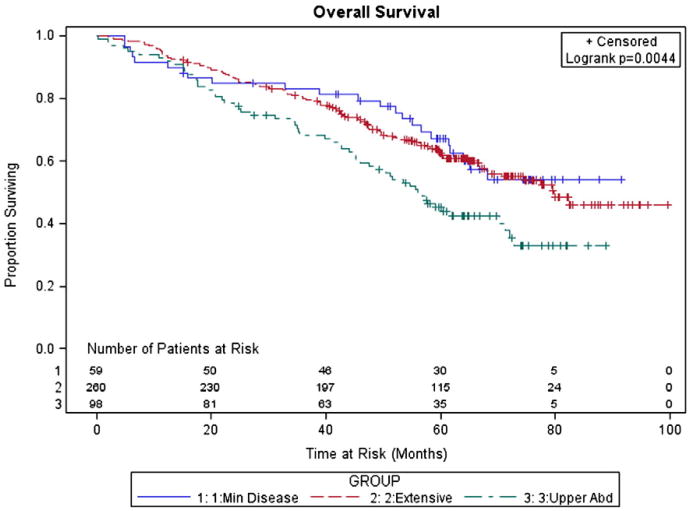
Methods: We reviewed data from 417 stage III EOC patients cytoreduced to microscopic disease and given adjuvant intravenous platinum/paclitaxel on one of three randomized Gynecologic Oncology Group (GOG) trials. We subdivided patients into three groups based on preoperative disease burden: (1) minimal disease (MD) defined by pelvic tumor and retroperitoneal metastasis (2) abdominal peritoneal disease (APD) with disease limited to the pelvis, retroperitoneum, lower abdomen and omentum; and (3) upper abdominal disease (UAD) with disease affecting the diaphragm, spleen, liver or pancreas. We assessed the survival impact of potential prognostic factors, focusing on initial disease distribution using a proportional hazards model and estimated Kaplan-Meier survival curves.
Results: The study groups had similar clinicopathologic characteristics. Median overall survival (OS) was not reached in MD patients compared to 80 and 56 months in the APD and UAD groups (P<0.05). The five-year survival percentages for MD, APD, and UAD were 67%, 63%, and 45%. In multivariate analysis, the UAD group had a significantly worse prognosis than MD and APD both individually and combined (Progression Free Survival (PFS) Hazards Ratio (HR) 1.44; P=0.008 and OS HR 1.77; P=0.0004 compared to MD+APD).
Conclusion: Stage III EOC patients with initial disease in the upper abdomen have a worse prognosis despite cytoreductive surgery to microscopic residual implying that factors beyond cytoreductive effort are important in predicting survival.
Published by Elsevier Inc.
Conflict of interest statement
Figures

Comment in
-
Implications of upper abdominal disease in advanced ovarian cancer after surgical cytoreduction and relation with tumor biology.Gynecol Oncol. 2011 Dec;123(3):615; author reply 616. doi: 10.1016/j.ygyno.2011.07.027. Epub 2011 Aug 11. Gynecol Oncol. 2011. PMID: 21839497 No abstract available.
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics, 2010. CA Cancer J Clin. 2010 - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. 2002;20:1248–59. - PubMed
-
- Fader AN, Rose PG. Role of surgery in ovarian carcinoma. J Clin Oncol. 2007;25:2873–83. - PubMed
-
- Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr. 1975;42:101–4. - PubMed
-
- Eisenkop SM, Spirtos NM, Lin WC. “Optimal” cytoreduction for advanced epithelial ovarian cancer: a commentary. Gynecol Oncol. 2006;103:329–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
