

Prevalence of infective endocarditis in patients with Staphylococcus aureus bacteraemia: the value of screening with echocardiography
- PMID: 21685200
- PMCID: PMC3117467
- DOI: 10.1093/ejechocard/jer023
Prevalence of infective endocarditis in patients with Staphylococcus aureus bacteraemia: the value of screening with echocardiography
Abstract
Aims: Staphylococcus aureus infective endocarditis (IE) is a critical medical condition associated with a high morbidity and mortality. In the present study, we prospectively evaluated the importance of screening with echocardiography in an unselected S. aureus bacteraemia (SAB) population.
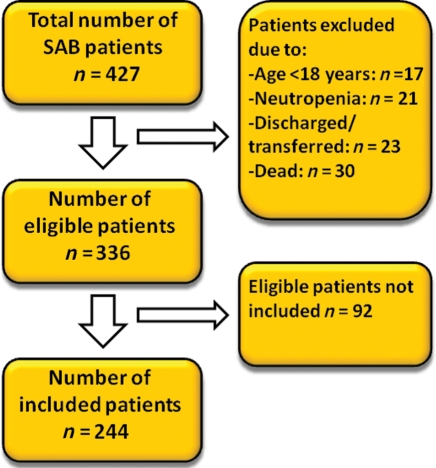
Methods and results: From 1 January 2009 to 31 August 2010, a total of 244 patients with SAB at six Danish hospitals underwent screening echocardiography. The inclusion rate was 73% of all eligible patients (n= 336), and 53 of the 244 included patients (22%; 95% CI: 17-27%) were diagnosed with definite IE. In patients with native heart valves the prevalence was 19% (95% CI: 14-25%) compared with 38% (95% CI: 20-55%) in patients with prosthetic heart valves and/or cardiac rhythm management devices (P= 0.02). No difference was found between Main Regional Hospitals and Tertiary Cardiac Hospitals, 20 vs. 23%, respectively (NS). The prevalence of IE in high-risk patients with one or more predisposing condition or clinical evidence of IE were significantly higher compared with low-risk patients with no additional risk factors (38 vs. 5%; P < 0.001). IE was associated with a higher 6 months mortality, 14(26%) vs. 28(15%) in SAB patients without IE, respectively (P < 0.05).
Conclusion: SAB patients carry a high risk for development of IE, which is associated with a worse prognosis compared with uncomplicated SAB. The presenting symptoms and clinical findings associated with IE are often non-specific and echocardiography should always be considered as part of the initial evaluation of SAB patients.
Comment in
-
Role of echocardiography in the evaluation of patients with Staphylococcus aureus bacteraemia: time to look at the heart.Eur J Echocardiogr. 2011 Jun;12(6):411-3. doi: 10.1093/ejechocard/jer067. Eur J Echocardiogr. 2011. PMID: 21685199 No abstract available.
References
-
- Biedenbach DJ, Moet GJ, Jones RN. Occurrence and antimicrobial resistance pattern comparisons among bloodstream infection isolates from the SENTRY Antimicrobial Surveillance Program (1997–2002) Diagn Microbiol Infect Dis. 2004;50:59–69. - PubMed
-
- Lyytikainen O, Ruotsalainen E, Jarvinen A, Valtonen V, Ruutu P. Trends and outcome of nosocomial and community-acquired bloodstream infections due to Staphylococcus aureus in Finland, 1995–2001. Eur J Clin Microbiol Infect Dis. 2005;24:399–404. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–54. - PubMed
-
- Abraham J, Mansour C, Veledar E, Khan B, Lerakis S. Staphylococcus aureus bacteremia and endocarditis: the Grady Memorial Hospital experience with methicillin-sensitive S aureus and methicillin-resistant S aureus bacteremia. Am Heart J. 2004;147:536–9. - PubMed
-
- Benfield T, Espersen F, Frimodt-Moller N, Jensen AG, Larsen AR, Pallesen LV, et al. Increasing incidence but decreasing in-hospital mortality of adult Staphylococcus aureus bacteraemia between 1981 and 2000. Clin Microbiol Infect. 2007;13:257–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous