

How reliable are tests for trachoma?--a latent class approach
- PMID: 21685340
- PMCID: PMC3176003
- DOI: 10.1167/iovs.11-7419
How reliable are tests for trachoma?--a latent class approach
Abstract
Purpose: Tests for ocular Chlamydia trachomatis have not been well characterized, because there is no gold standard test. Latent class analysis (LCA) was performed to estimate the sensitivity and specificity of laboratory and clinical tests for trachoma in the absence of a gold standard.
Methods: Individual data from pretreatment, hyperendemic areas in Ethiopia were used. A clustered LCA was performed for three diagnostic tests: PCR and WHO simplified criteria grades of follicular trachoma (TF) and intense trachomatous inflammation (TI).
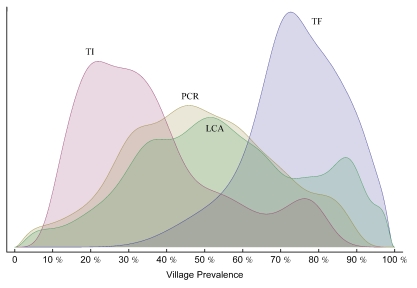
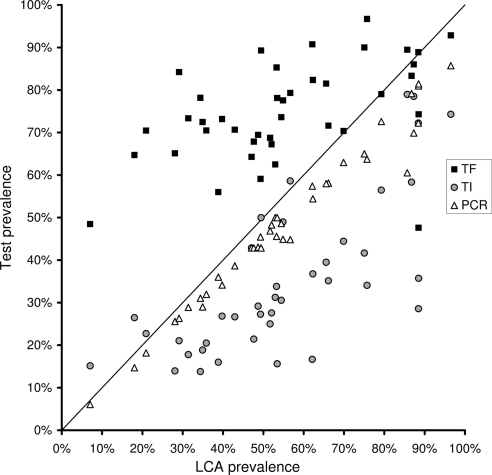
Results: Data from 2111 subjects in 40 villages were available. TF was estimated to be 87.3% (95% CI, 83.3-90.1) sensitive and 36.6% (95% CI, 23.6-40.3) specific; TI was estimated to be 53.6% (95% CI, 46.1-88.0) sensitive and 88.3% (95% CI, 83.3-92.0) specific, and PCR was estimated to be 87.5% (95% CI, 79.9-97.2) sensitive and 100% (95% CI 69.3-100) specific.
Conclusions: LCA allows for an estimate of test characteristics without prior assumption of their performance. TF and TI were found to act in a complementary manner: TF is a sensitive test and TI is a specific test. PCR is highly specific but lacks sensitivity. The performance of these tests may be due to the time course of ocular chlamydial infection, and for this reason, results may differ in areas of low prevalence or recent mass treatment (ClinicalTrials.gov number, NCT00221364).
Figures
References
-
- Schachter J, West SK, Mabey D, et al. Azithromycin in control of trachoma. Lancet. 1999;354(9179):630–635 - PubMed
-
- World Health Organization Report of the Eighth Meeting of the WHO Alliance for the Global Elimination of Blinding Trachoma. Geneva, WHO; 2004
-
- Lietman T, Porco T, Dawson C, Blower S. Global elimination of trachoma: how frequently should we administer mass chemotherapy? Nat Med. 1999;5(5):572–576 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
