

doi: 10.1136/bcr.11.2008.1198.
Epub 2009 Mar 17.
Neuroimaging in subclavian steal syndrome
Affiliations
- PMID: 21686421
- PMCID: PMC3027939
- DOI: 10.1136/bcr.11.2008.1198
Item in Clipboard
Neuroimaging in subclavian steal syndrome
BMJ Case Rep.
2009.
No abstract available
Figures
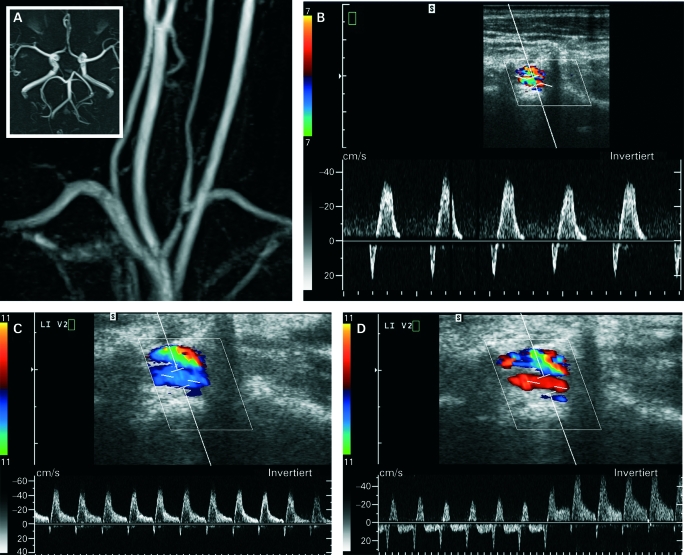
(A) Contrast-enhanced MRI/angiography of the supra-aortal arteries showing moderate left subclavian artery stenosis and unremarkable finding on time-of-flight MR-angiography of the intracranial vessels. (B) Doppler and duplex Doppler sonography showing a bidirectional wave-form with initial antegrade flow and subsequent retrograde flow in the V2 segment of the left vertebral artery. (C) Retrograde flow was increased at manual work and (D) was markedly increased after release of a pressure cuff on the left arm.

(A) Digital subtraction angiography showing moderate stenosis of the left subclavian artery; however, with dilatation at the origin of the left vertebral artery, (B) retrograde and weak contrast filling of the left vertebral artery also into the cervical segments in the later phase (C). (D) Blood flow was significantly increased after left subclavian artery stenting.

MRI of the brain showing hyperintense lesions of the occipital lobe on fluid-attenuated inversion recovery (FLAIR) (A, arrows) and diffusion weighted imaging (DWI) (B, arrows) sequences; MR-angiography (C) showing patent subclavian, basilar and vertebral arteries, but abnormal flow in the left V4 segment (D, arrow).

(A) Colour duplex sonography indicated retrograde flow in the V1 segment with vertebral vein running parallel to the artery. The Doppler spectrum showed a short orthograde flow with flow reversal and high negative flow in end diastolic. (B) Flow oscillation in the V3 segment with diminishment of the orthograde component in the Doppler spectrum. (C) Complete flow reversal (in red) in the left V4 segment with normal flow in the right V4 segment (in blue). (D) Colour duplex sonography of the brachial artery with high flow and spectral broadening. The calculated flow volume was 3945 ml/min. (E) Compression of the arteriovenous fistula caused cessation of retrograde flow and increase of the orthograde flow in the V1 segment (white arrow). (F) Compression of the arteriovenous fistula ended retrograde flow in the left V4 segment; however, orthograde flow could not be detected.
References
-
- Schenk WG., 3rd Subclavian steal syndrome from high-output brachiocephalic arteriovenous fistula: a previously undescribed complication of dialysis access. J Vasc Surg 2001; 33: 883–5 - PubMed
-
- Wu C, Zhang J, Ladner CJ, et al. Subclavian steal syndrome: diagnosis with perfusion metrics from contrast-enhanced MR angiographic bolus-timing examination—initial experience. Radiology 2005; 235: 927–33 - PubMed
LinkOut - more resources
Full Text Sources