

Benign endoscopic biopsies may be a red herring
- PMID: 21686577
- PMCID: PMC3030219
- DOI: 10.1136/bcr.09.2008.0894
Benign endoscopic biopsies may be a red herring
Abstract
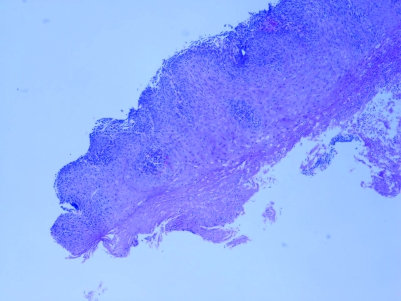
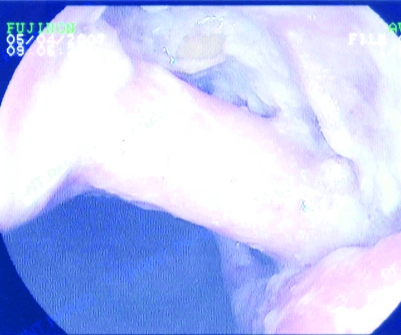
A 64-year-old man presented with haematemesis and melena. Repeated endoscopies showed extensive candidiasis with an exophytic mass like a shelf of tumour. Biopsies showed chronic inflammatory changes with candidiasis without evidence of malignancy. His only complaint was feeling tired and loss of energy. There was no dysphagia but slight retrostenal discomfort on swallowing. Computed tomography scan reported an opacification in the right upper lobe adjacent to the mediastinum. This contained air bronchograms and several irregular air filled cavities. There was significant mediastinal adenopathy. Two endoscopies were done after that and both of them demonstrated a fistulous connection with the bronchial tree. Biopsies failed to show any neoplasm. The patient underwent a three stage oesophagectomy with removal of the adjacent lung lobe and a reconstructive procedure. The resected mass was sent for histopathology which showed a well differentiated squamous cell carcinoma of the oesophagus which locally invaded the lung.
Figures








References
-
- . Case of records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 22–2000. A 74-year-old man with unrelenting dysphagia. N Engl J Med 2000; 343: 199–205 - PubMed
-
- Pohl D, Tutuian R: Achalasia: an overview of diagnosis and treatment. J Gastrointestin Liver Dis 2007; 16: 297–303 - PubMed
-
- Kahrilas PJ, Kishk SM, Helm JF, et al. Comparison of pseudoachalasia and achalasia. Am J Med 1987; 82: 439–46 - PubMed
-
- Gockel I, Eckardt VF, Schmitt T, et al. Pseudoachalasia: a case series and analysis of the literature. Scand J Gastroenterol 2005; 40: 378–85 - PubMed
-
- Tucker HJ, Snape WJ, Jr, Cohen S. Achalasia secondary to carcinoma: manometric and clinical features. Ann Intern Med 1978; 89: 315–8 - PubMed
LinkOut - more resources
Full Text Sources