

Boerhaave syndrome: a diagnostic conundrum
- PMID: 21686835
- PMCID: PMC3027424
- DOI: 10.1136/bcr.07.2008.0375
Boerhaave syndrome: a diagnostic conundrum
Abstract
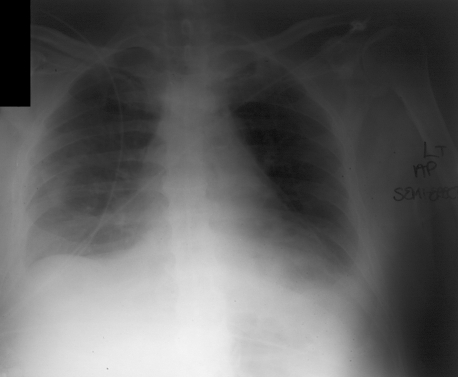
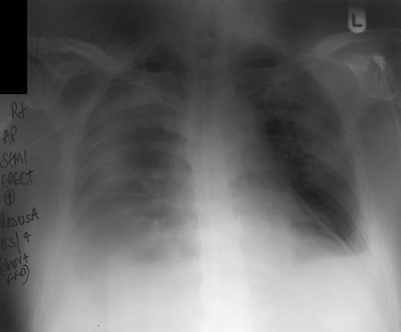
A 79-year-old man presented to the Emergency Department with abdominal pain 1 day after an elective total knee replacement. The patient was confused and drowsy, with a high fever, hypotension and uncontrolled atrial fibrillation. He subsequently developed respiratory failure, requiring admission to intensive care. It was then noted that a large pleural effusion had developed between two chest radiographs performed only 4 h apart. A pigtail catheter inserted into the pleural space revealed a transudate of pH 7.0 with an amylase of 17 220 U (serum amylase 54 U), and thus a diagnosis of spontaneous oesophageal rupture or Boerhaave syndrome was made. Despite drainage of the pleural space, the patient developed shock and multiorgan failure requiring mechanical ventilation, renal replacement therapy and cardiovascular support. The oesophageal leak was treated conservatively with intercostal tube drainage; the patient made a full recovery and was discharged from hospital 75 days later.
Figures

References
-
- Wolfson D, Barkin JS. Treatment of Boerhaave’s syndrome. Curr Treat Options Gastroenterol 2007; 10: 71–7 - PubMed
-
- Lemke T, Jagminas L. Spontaneous oesophageal rupture: a frequently missed diagnosis. Am Surg 1999; 65: 449–52 - PubMed
-
- Henderson JA, Peloquin AJ. Boerhaave revisited: spontaneous oesophageal perforation as a diagnostic masquerader. Am J Med 1989; 86: 559–67 - PubMed
-
- Brauer RB, Liebermann-Meffert D, Stein HJ, et al. Boerhaave’s syndrome: analysis of the literature and report of new cases. Dis Esophagus 1997; 10: 64–8 - PubMed
-
- Jougon J, McBride T, Delcambre F, et al. Primary oesophageal repair for Boerhaave’s syndrome whatever the free interval between perforation and treatment. Eur J Cardiothoracic Surg 2004; 25: 475–9 - PubMed
LinkOut - more resources
Full Text Sources