

Giant right atrial cystic hamartoma: a case report and literature review
- PMID: 21686985
- PMCID: PMC3029438
- DOI: 10.1136/bcr.02.2009.1587
Giant right atrial cystic hamartoma: a case report and literature review
Abstract
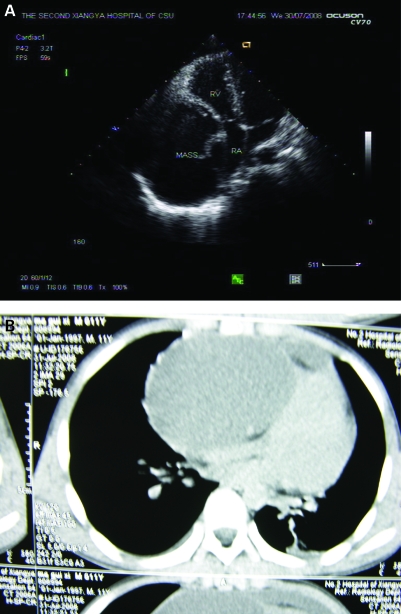
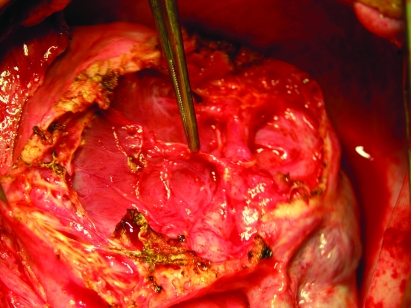
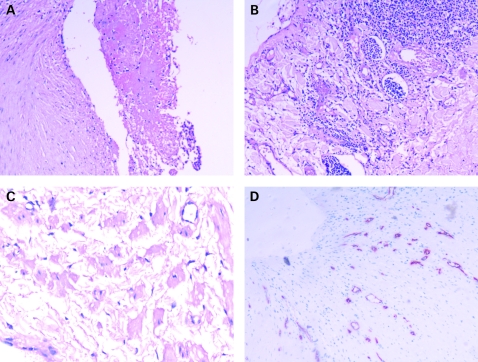
An 11-year-old boy presenting with palpitation and chest distress was found to have gross cardiomegaly on chest radiography. Subsequent echocardiography revealed an intramural giant cystic mass in the right atrium. An operative measure was planned to prevent acute cardiac tamponade and right coronary artery obstruction. The patient successfully underwent open cystectomy to remove the mass, which was located on the front wall of the right atrium and extended to the atrioventricular appendage. Histopathological examination confirmed a cystic hamartoma. To the best of our knowledge, this is the first reported case of a giant cystic hamartoma located on the right atrium.
Trial registration number: 704640.
Figures
References
-
- Sarjeant JM, Butany J, Cusimano RJ. Cancer of the heart: epidemiology and management of primary tumors and metastases. Am J Cardiovasc Drugs 2003; 3: 407–21 - PubMed
-
- Reynen K, Köckeritz U, Strasser RH. Metastases to the heart. Ann Oncol 2004; 15: 375–81 - PubMed
-
- Fealey ME, Edwards WD, Miller DV, et al. Hamartomas of mature cardiac myocytes: report of 7 new cases and review of literature. Hum Pathol 2008; 39: 1064–71 - PubMed
-
- Saffitz JE, Ferrans VJ, Rodriguez ER, et al. Histiocytoid cardiomyopathy: a cause of sudden death in apparently healthy infants. Am J Cardiol 1983; 52: 215–7 - PubMed
-
- Kearney DL, Titus JL, Hawkins EP, et al. Pathologic features of myocardial hamartomas causing childhood tachyarrhythmias. Circulation 1987; 75: 705–10 - PubMed
LinkOut - more resources
Full Text Sources