

The natural history of nonalcoholic fatty liver disease with advanced fibrosis or cirrhosis: an international collaborative study
- PMID: 21688282
- PMCID: PMC3238674
- DOI: 10.1002/hep.24491
The natural history of nonalcoholic fatty liver disease with advanced fibrosis or cirrhosis: an international collaborative study
Abstract
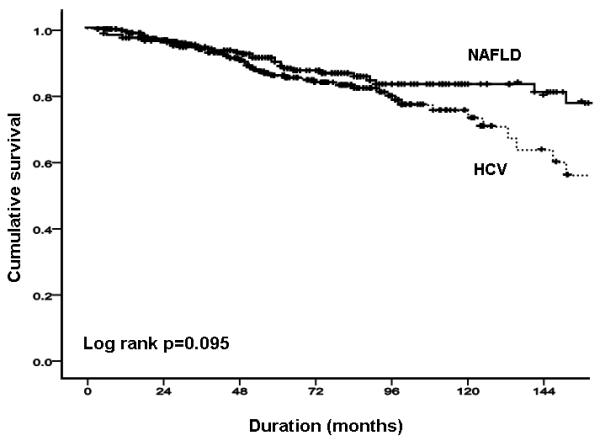
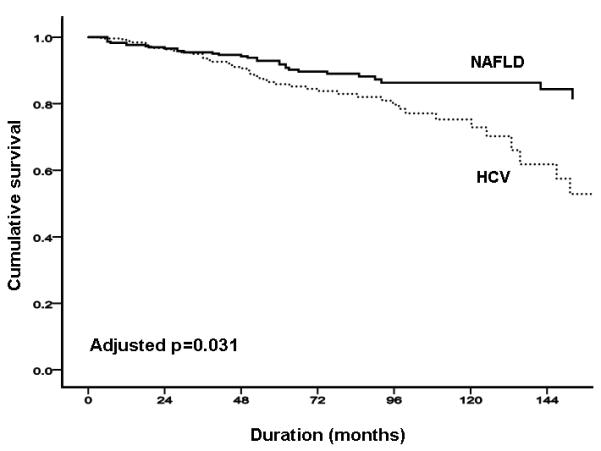
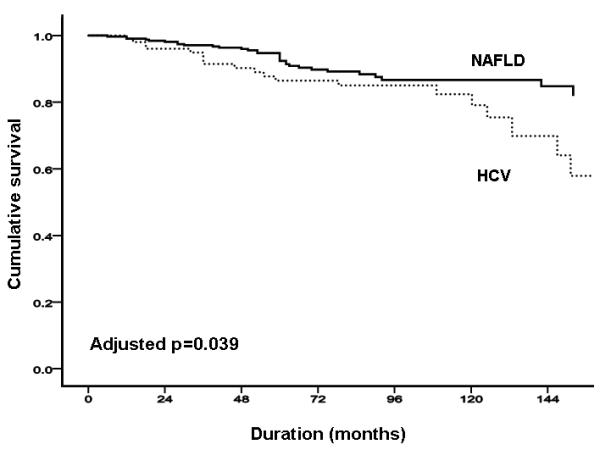
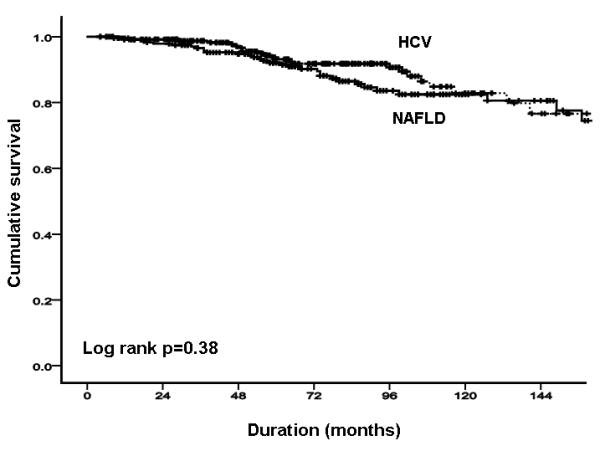
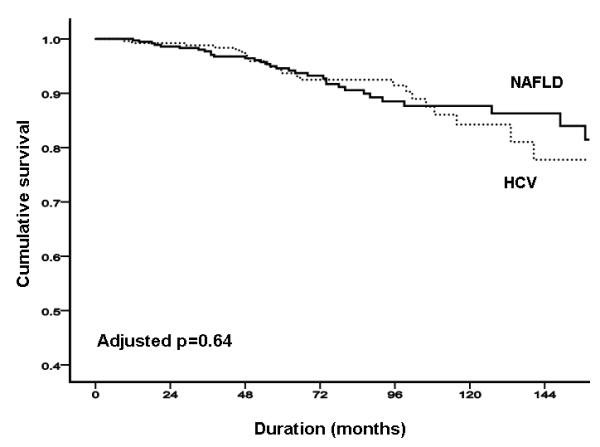
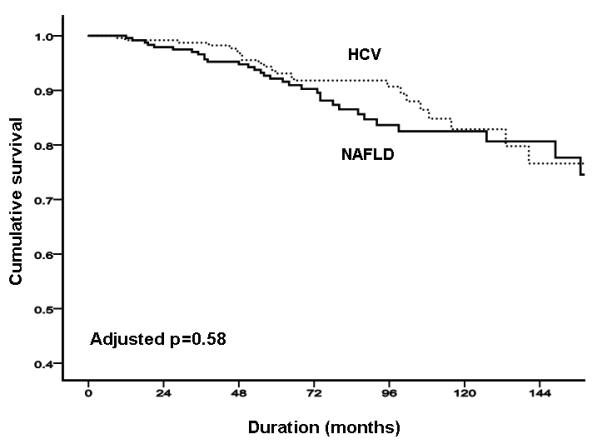
Information on the long-term prognosis of nonalcoholic fatty liver disease (NAFLD) is limited. We sought to describe the long-term morbidity and mortality of patients with NAFLD with advanced fibrosis or cirrhosis by prospectively studying 247 such patients from four international centers (in Australia, USA, UK and Italy). Their natural history was then compared with 264 patients with HCV infection who were either naïve or non-responders to treatment. Both cohorts were Child-Pugh class A and had advanced fibrosis (stage 3) or cirrhosis (stage 4) confirmed by liver biopsy at enrollment. In the NAFLD cohort, followed up for a mean of 85.6 months (range, 6-297), there were 48 (19.4%) liver-related complications and 33 (13.4%) deaths or liver transplants. In the HCV cohort, followed up for 74.9 months (mean; range, 6-238), there were 47 (16.7%) liver-related complications and 25 (9.4%) deaths or liver transplants. When adjusting for baseline differences in age and gender, the cumulative incidence of liver-related complications was lower in the NAFLD than the HCV cohort (P = 0.03), including incident hepatocellular cancer (6 versus 18; P = 0.03), but that of cardiovascular events (P = 0.17) and overall mortality (P = 0.6) were similar in both groups. In the NAFLD cohort, platelet count, stage 4 fibrosis, lowered platelet count, and lowered serum cholesterol and alanine aminotransferase (ALT) levels were associated with liver-related complications; an aspartate aminotransferase/ALT ratio >1 and older age were associated with overall mortality, and higher serum bilirubin levels and stage 4 fibrosis were associated with liver-related mortality.
Conclusions: Patients with NAFLD with advanced fibrosis or cirrhosis have lower rates of liver-related complications and hepatocellular cancer than corresponding patients with HCV infection, but similar overall mortality. Some clinical and laboratory features predict liver-related complications and other outcomes in patients with NAFLD.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures
Comment in
-
Will the increased prevalence of nonalcoholic steatohepatitis (NASH) in the age of better hepatitis C virus therapy make NASH the deadlier disease?Hepatology. 2011 Oct;54(4):1118-20. doi: 10.1002/hep.24634. Hepatology. 2011. PMID: 21956705 No abstract available.
References
-
- Argo CK, Caldwell SH. Epidemiology and natural history of non-alcoholic steatohepatitis. Clin Liver Dis. 2009 Nov;13(4):511–531. - PubMed
-
- Angulo P. GI epidemiology: nonalcoholic fatty liver disease. Aliment Pharmacol Ther. 2007 Apr 15;25(8):883–889. - PubMed
-
- Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002 Apr 18;346(16):1221–1231. - PubMed
-
- Bhala N, Usherwood T, George J. Non-alcoholic fatty liver disease. BMJ. 2009;339:b2474. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical