

Liver transplant recipient survival benefit with living donation in the model for endstage liver disease allocation era
- PMID: 21688284
- PMCID: PMC3184197
- DOI: 10.1002/hep.24494
Liver transplant recipient survival benefit with living donation in the model for endstage liver disease allocation era
Abstract
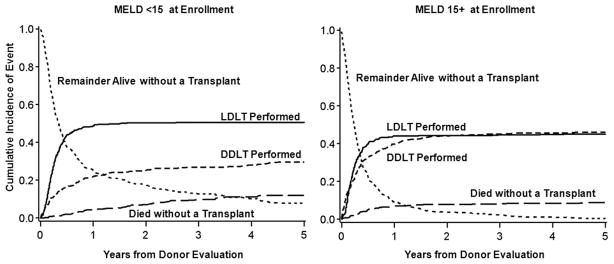
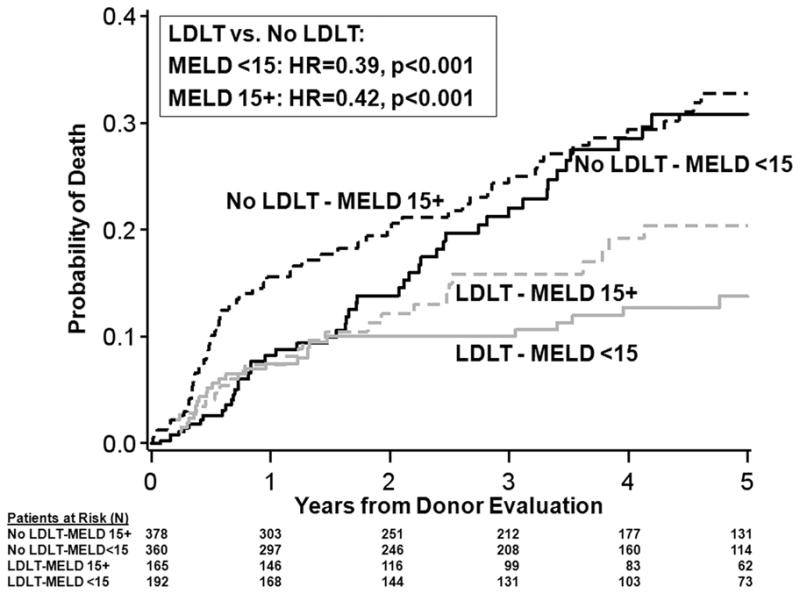
Receipt of a living donor liver transplant (LDLT) has been associated with improved survival compared with waiting for a deceased donor liver transplant (DDLT). However, the survival benefit of liver transplant has been questioned for candidates with Model for Endstage Liver Disease (MELD) scores <15, and the survival advantage of LDLT has not been demonstrated during the MELD allocation era, especially for low MELD patients. Transplant candidates enrolled in the Adult-to-Adult Living Donor Liver Transplantation Cohort Study after February 28, 2002 were followed for a median of 4.6 years. Starting at the time of presentation of the first potential living donor, mortality for LDLT recipients was compared to mortality for patients who remained on the waiting list or received DDLT (no LDLT group) according to categories of MELD score (<15 or ≥ 15) and diagnosis of hepatocellular carcinoma (HCC). Of 868 potential LDLT recipients (453 with MELD <15; 415 with MELD ≥ 15 at entry), 712 underwent transplantation (406 LDLT; 306 DDLT), 83 died without transplant, and 73 were alive without transplant at last follow-up. Overall, LDLT recipients had 56% lower mortality (hazard ratio [HR] = 0.44, 95% confidence interval [CI] 0.32-0.60; P < 0.0001). Among candidates without HCC, mortality benefit was seen both with MELD <15 (HR = 0.39; P = 0.0003) and MELD ≥ 15 (HR = 0.42; P = 0.0006). Among candidates with HCC, a benefit of LDLT was not seen for MELD <15 (HR = 0.82, P = 0.65) but was seen for MELD ≥ 15 (HR = 0.29, P = 0.043).
Conclusion: Across the range of MELD scores, patients without HCC derived a significant survival benefit when undergoing LDLT rather than waiting for DDLT in the MELD liver allocation era. Low MELD candidates with HCC may not benefit from LDLT.
Copyright © 2011 American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
Comment in
-
Benefit of living donor liver transplantation: who and when?Hepatology. 2011 Oct;54(4):1125-6. doi: 10.1002/hep.24578. Hepatology. 2011. PMID: 21800337 No abstract available.
References
-
- Sarasin FP, Majno PE, Llovet JM, et al. Living donor liver transplantation for early hepatocellular carcinoma: A life-expectancy and cost-effectiveness perspective. Hepatology. 2001;33:1703–1709. - PubMed
-
- Cheng SJ, Pratt DS, Freeman RB, Jr, et al. Living-donor versus cadaveric liver transplantation for non-resectable small hepatocellular carcinoma and compensated cirrhosis: A decision analysis. Transplantation. 2001;72:861–868. - PubMed
-
- Merion RM, Schaubel DE, Dyskstra DM, et al. The survival benefit of liver transplantation. Am J Transplant. 2005;5:307–313. - PubMed