

A randomized, pilot trial of etanercept in dermatomyositis
- PMID: 21688301
- PMCID: PMC3170432
- DOI: 10.1002/ana.22477
A randomized, pilot trial of etanercept in dermatomyositis
Abstract
Objective: The aims of this pilot study were to assess (1) the safety and tolerability of etanercept in dermatomyositis (DM); (2) the feasibility and safety of a forced prednisone taper; and (3) outcome measures, including those recommended by the International Myositis Assessment Clinical Study (IMACS) group.
Methods: We conducted a randomized, double-blind, placebo-controlled trial of etanercept (50mg subcutaneously weekly) for 52 weeks in DM subjects. Subjects were tapered off prednisone in a standardized schedule as tolerated over the initial 24 weeks of the study. Principal outcomes included adverse events, time from randomization to treatment failure (inability to wean off prednisone on schedule), and average prednisone dosage after week 24.
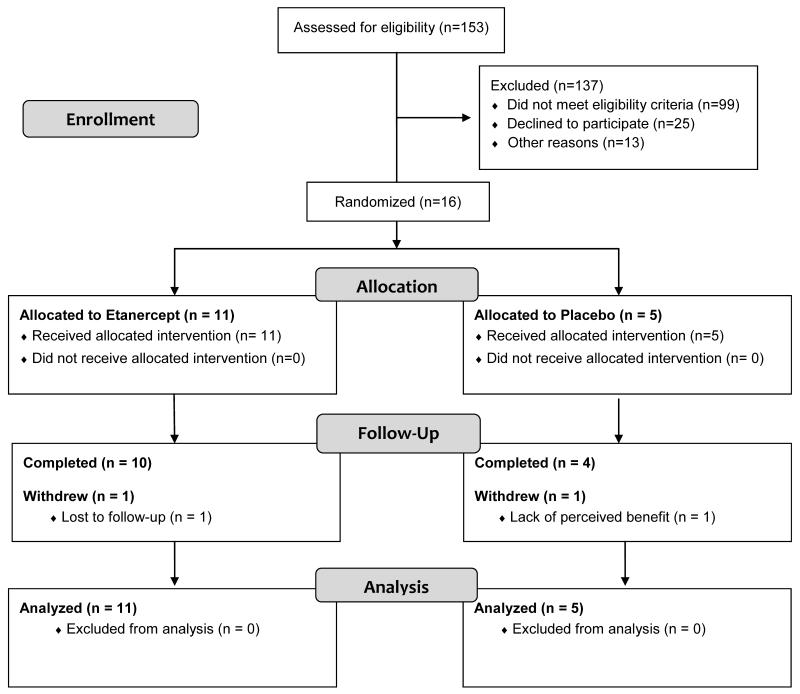
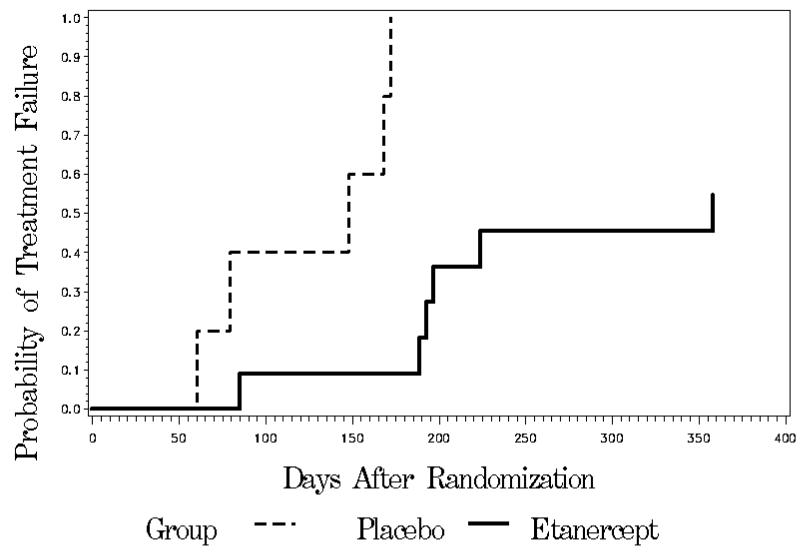
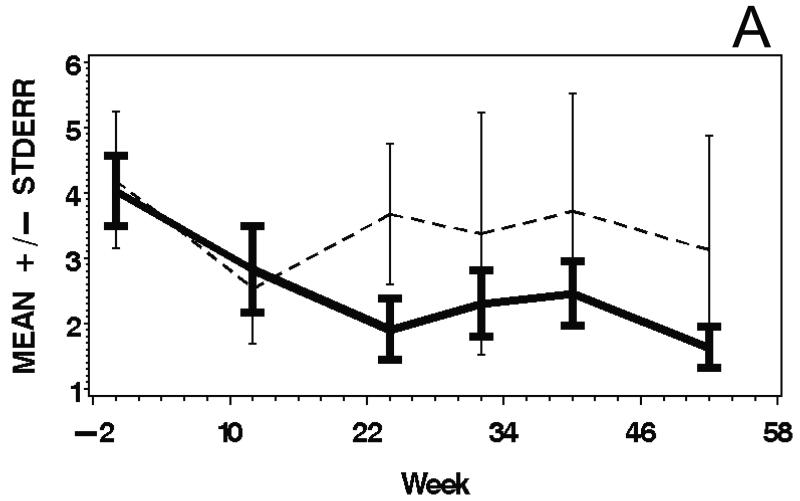
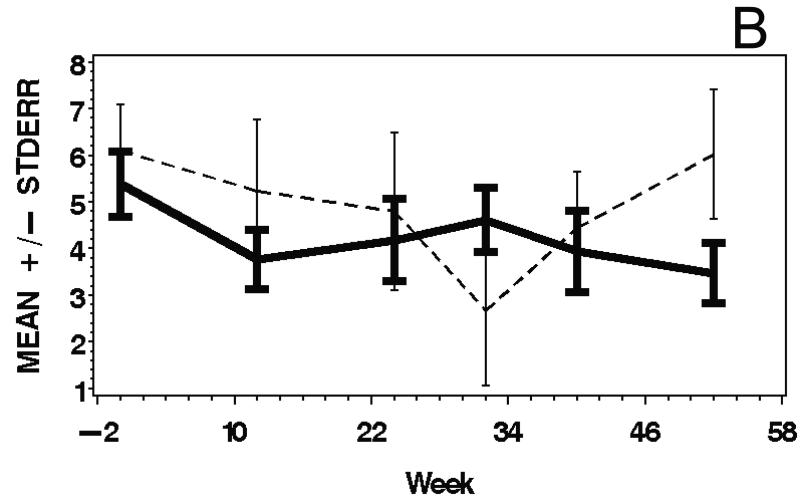
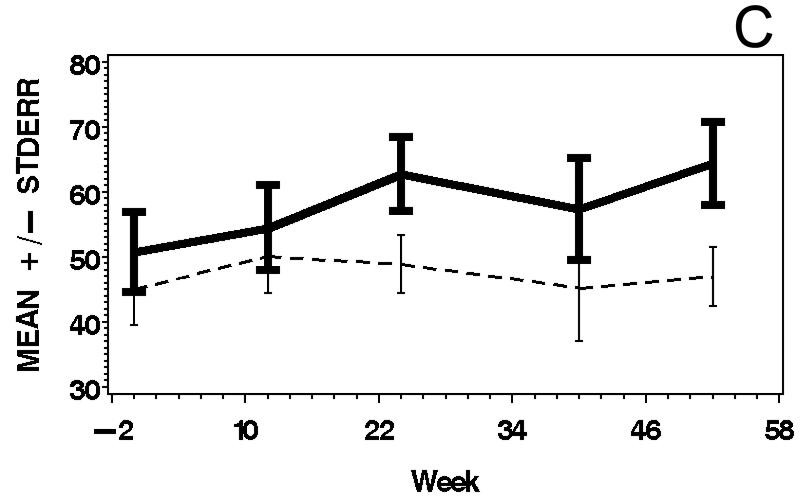
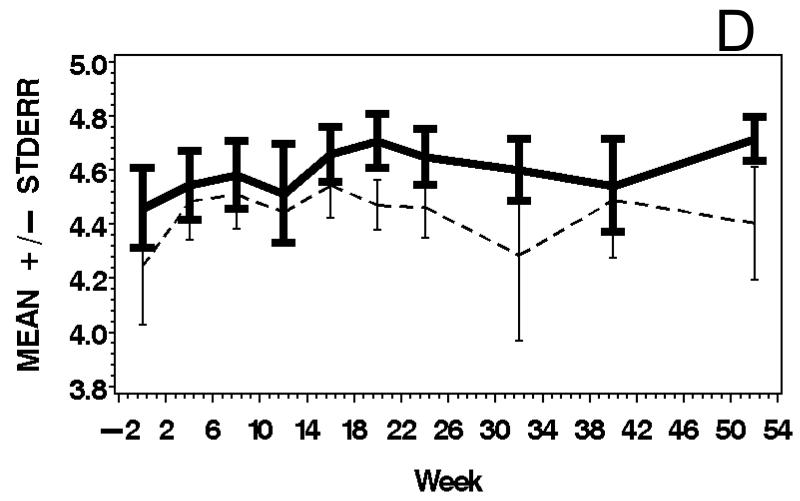
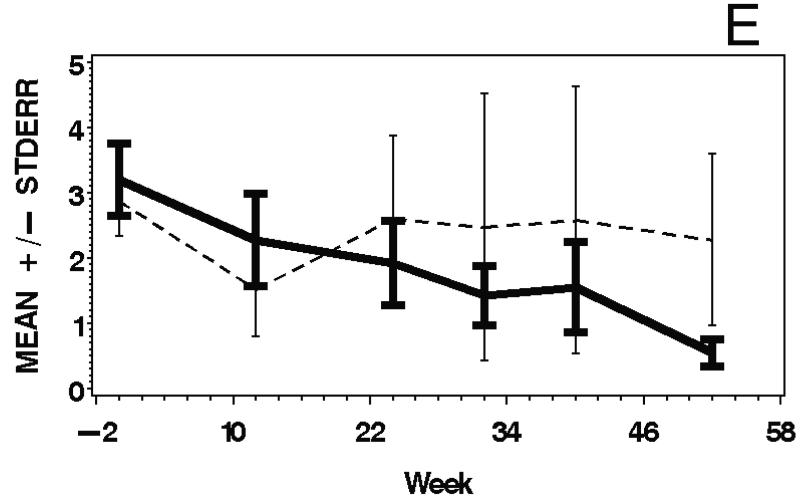
Results: Sixteen subjects were randomized, 11 to etanercept and 5 to placebo. There were no significant differences in adverse event rates between the treatment groups, although 5 etanercept-treated and 1 placebo-treated subjects developed worsening rash. All 5 subjects receiving placebo were treatment failures (median time to treatment failure 148 days). In contrast, 5 of 11 subjects in the etanercept arm were successfully weaned off prednisone; the median time to treatment failure in this group was 358 days (p = 0.0002). The median of the average prednisone dosage after week 24 was 29.2mg/day in the placebo group and 1.2mg/day in the etanercept group (p = 0.02). IMACS and other outcome measures demonstrated excellent test-retest reliability (intraclass correlation coefficients 0.79-0.99). There was no significant treatment effect on functional outcome.
Interpretation: The findings of no major safety concerns and a steroid-sparing effect in our study suggest that further investigation of etanercept as a treatment for DM is warranted.
Trial registration: ClinicalTrials.gov NCT00282880.
Copyright © 2011 American Neurological Association.
Figures
Comment in
-
Etanercept as steroid-sparing agent in dermatomyositis.Ann Neurol. 2011 Oct;70(4):670-1; author reply 671-2. doi: 10.1002/ana.22624. Ann Neurol. 2011. PMID: 22028232 No abstract available.
References
-
- Amato AA, Barohn RJ. Evaluation and treatment of inflammatory myopathies. J Neurol Neurosurg Psychiatry. 2009;80:1060–1068. - PubMed
-
- DeBleeker JL, Meire VI, Declercq W, Van Aken EH. Immunolocalization of tumor necrosis factor-alpha and its receptors in inflammatory myopathies. Neuromusc Dis. 1999;9:239–246. - PubMed
-
- DeBleeker JL, Engel AG. Expression of cell adhesion molecules in inflammatory myopathies and Duchenne dystrophy. J Neuropathol Exp Neurol. 1994;53:369–376. - PubMed
-
- Fedcyyna TO, Lutz J, Pachman LM. Expression of TNFα by muscle fibers in biopsies from children with untreated juvenile dermatomyositis: association with the TNF-α allele. Clin Immunol. 2001;100:236–239. - PubMed
-
- Kuru S, Inukai A, Liang Y, Doyu M, Takano A, Sobue G. Tumor necrosis factor-α expression in muscles of polymyositis and dermatomyositis. Acta Neuropathol (Berl) 2000;99:585–588. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
