

Capacity building permitting comprehensive monitoring of a severe case of Lassa hemorrhagic fever in Sierra Leone with a positive outcome: case report
- PMID: 21689444
- PMCID: PMC3283910
- DOI: 10.1186/1743-422X-8-314
Capacity building permitting comprehensive monitoring of a severe case of Lassa hemorrhagic fever in Sierra Leone with a positive outcome: case report
Abstract
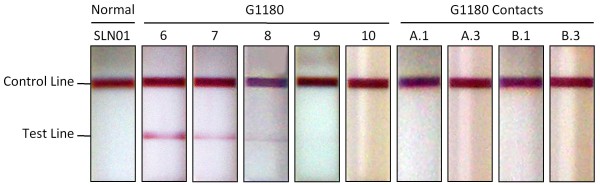
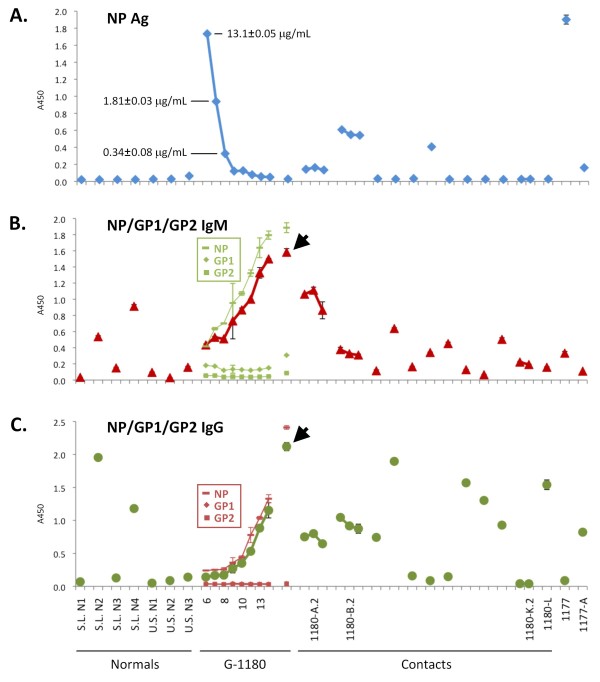
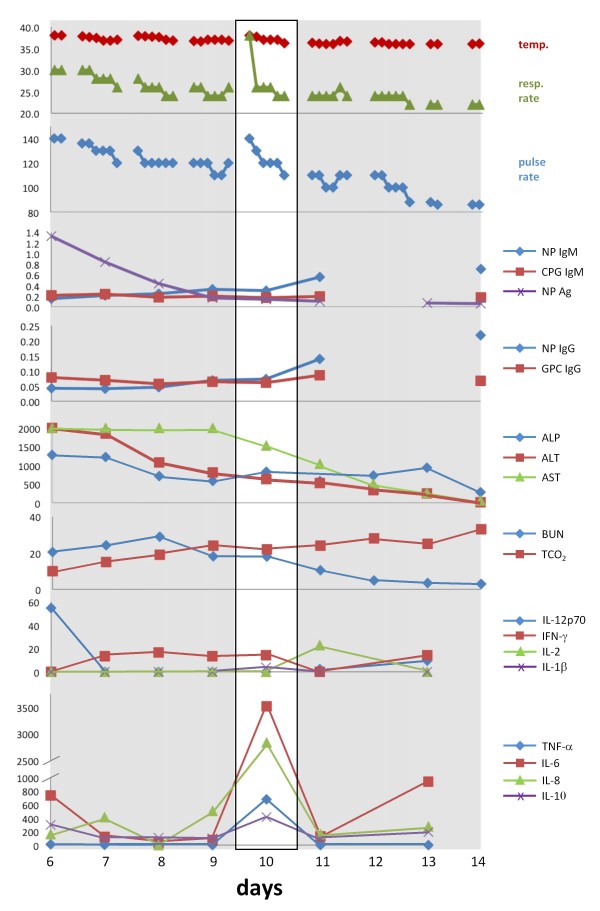
Lassa fever is a neglected tropical disease with a significant impact on the health care system of endemic West African nations. To date, case reports of Lassa fever have focused on laboratory characterisation of serological, biochemical and molecular aspects of the disease imported by infected individuals from Western Africa to the United States, Canada, Europe, Japan and Israel. Our report presents the first comprehensive real time diagnosis and characterization of a severe, hemorrhagic Lassa fever case in a Sierra Leonean individual admitted to the Kenema Government Hospital Lassa Fever Ward. Fever, malaise, unresponsiveness to anti-malarial and antibiotic drugs, followed by worsening symptoms and onset of haemorrhaging prompted medical officials to suspect Lassa fever. A recombinant Lassa virus protein based diagnostic was employed in diagnosing Lassa fever upon admission. This patient experienced a severe case of Lassa hemorrhagic fever with dysregulation of overall homeostasis, significant liver and renal system involvement, the interplay of pro- and anti-inflammatory cytokines during the course of hospitalization and an eventual successful outcome. These studies provide new insights into the pathophysiology and management of this viral illness and outline the improved infrastructure, research and real-time diagnostic capabilities within LASV endemic areas.
Figures
References
-
- Buckley SM, Casals J. Lassa fever, a new virus disease of man from West Africa. 3. Isolation and characterization of the virus. Am J Trop Med Hyg. 1970;19(4):680–91. - PubMed
-
- Birmingham K, Kenyon G. Lassa fever is unheralded problem in West Africa. Nat Med. 2001;7(8):878.. - PubMed
-
- Fisher-Hoch SP, McCormick JB. Lassa fever vaccine: A review. Expert Rev Vaccines. 2004;3:103–111. - PubMed
-
- McCormick JB. Epidemiology and control of Lassa fever. Current Topics in Microbiol and Immunol. 1987;134:69–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
