

Hilar cholangiocarcinoma: tumor depth as a predictor of outcome
- PMID: 21690446
- PMCID: PMC3308171
- DOI: 10.1001/archsurg.2011.122
Hilar cholangiocarcinoma: tumor depth as a predictor of outcome
Abstract
Background: The American Joint Committee on Cancer staging system for hilar cholangiocarcinoma may be inaccurate because the bile duct lacks discrete tissue boundaries.
Objectives: To examine the accuracy of the American Joint Committee on Cancer staging schemes and to determine the prognostic implications of tumor depth.
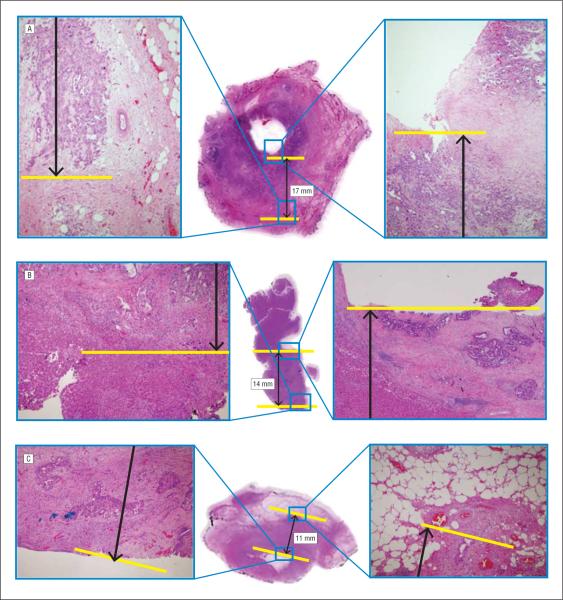
Design, setting, and patients: From January 1, 1987, through December 31, 2009, there were 106 patients who underwent resection of hilar cholangiocarcinoma who had pathologic slides available for re-review.
Main outcome measures: Tumor depth and overall survival.
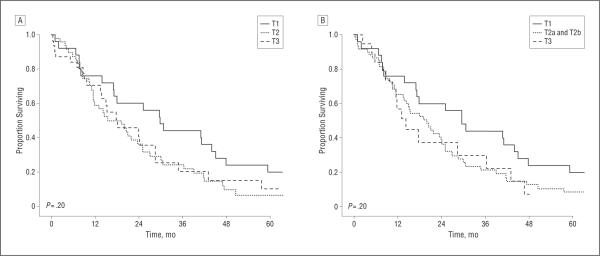
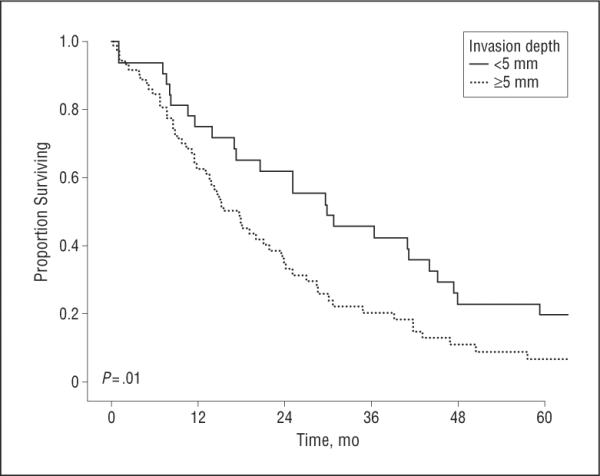
Results: Overall median survival was 19.9 months. The 6th and 7th editions of the T-classification criteria were unable to discriminate among T1, T2, and T3 lesions (P > .05 for all). Median survival was associated with the invasion depth of the tumor (≥5 mm vs <5 mm): 18 months vs 30 months (P = .01). On multivariate analysis, tumor depth remained predictive of disease-specific death (hazard ratio, 1.70; P = .03).
Conclusions: The American Joint Committee on Cancer T-classification criteria did not stratify patients with regard to prognosis. Depth of tumor invasion is a better predictor of long-term outcome.
Figures
References
-
- Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis: an unusual tumor with distinctive clinical and pathological features. Am J Med. 1965;38:241–256. - PubMed
-
- Altemeier WA, Gall EA, Zinninger MM, Hoxworth PI. Sclerosing carcinoma of the major intrahepatic bile ducts. AMA Arch Surg. 1957;75(3):450–460. - PubMed
-
- Ito F, Cho CS, Rikkers LF, Weber SM. Hilar cholangiocarcinoma: current management. Ann Surg. 2009;250(2):210–218. - PubMed
-
- Jarnagin WR. Cholangiocarcinoma of the extrahepatic bile ducts. Semin Surg Oncol. 2000;19(2):156–176. - PubMed
-
- Zervos EE, Osborne D, Goldin SB, et al. Stage does not predict survival after resection of hilar cholangiocarcinomas promoting an aggressive operative approach. Am J Surg. 2005;190(5):810–815. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
