

Pancreatic endocrine tumors with major vascular abutment, involvement, or encasement and indication for resection
- PMID: 21690450
- PMCID: PMC3122162
- DOI: 10.1001/archsurg.2011.129
Pancreatic endocrine tumors with major vascular abutment, involvement, or encasement and indication for resection
Abstract
Background: Surgery for pancreatic endocrine tumors (PETs) with blood vessel involvement is controversial.
Hypothesis: Resection of PETs with major blood vessel involvement can be beneficial.
Design: The combined databases of the National Institutes of Health and Stanford University hospitals were queried.
Main outcome measures: Operation, pathologic condition, complications, and disease-free and overall survival.
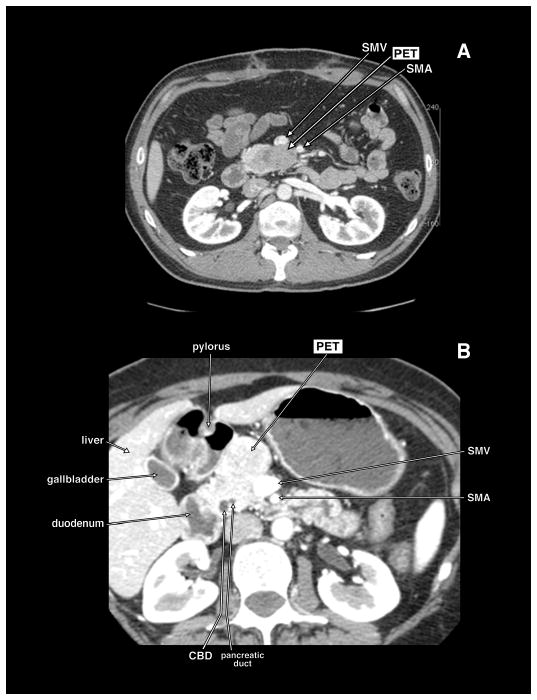
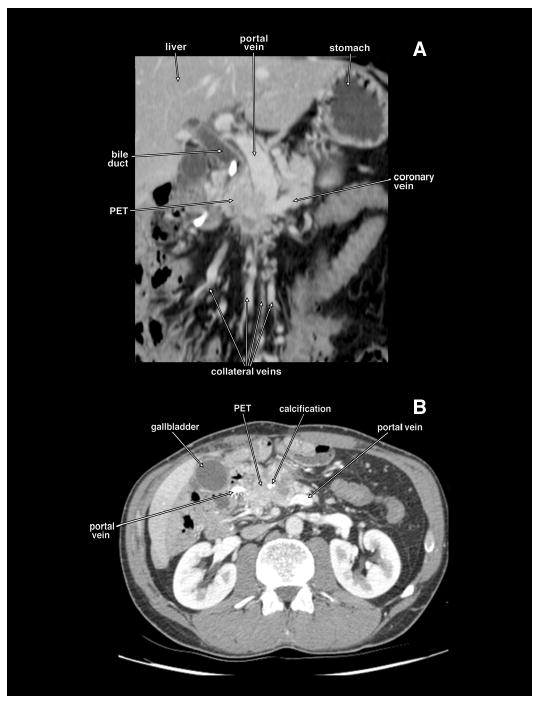
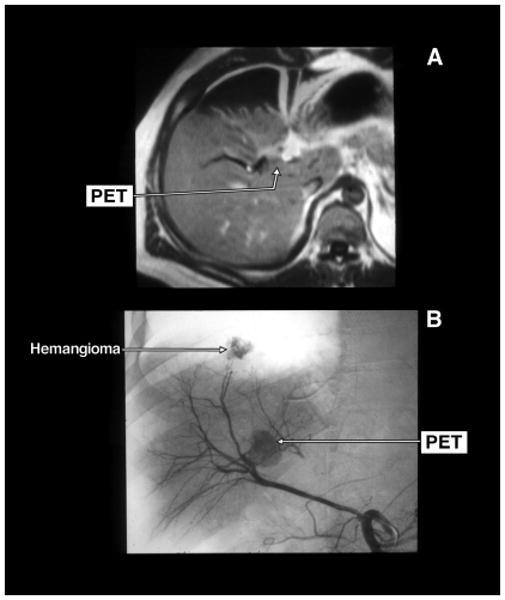
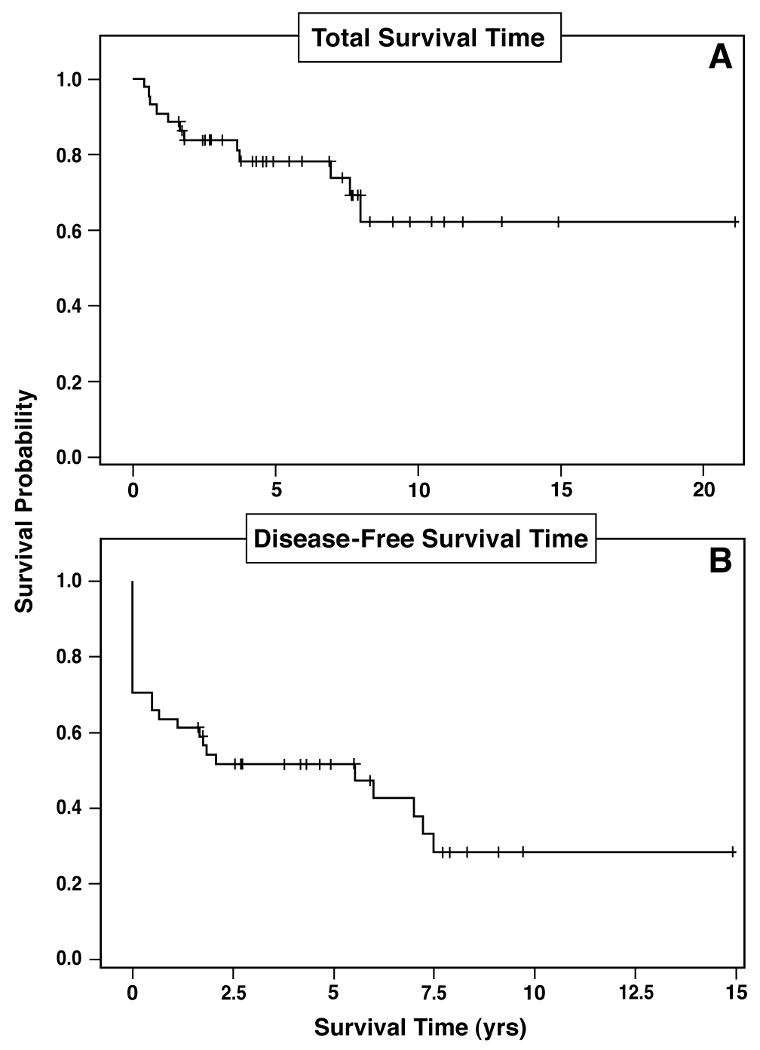
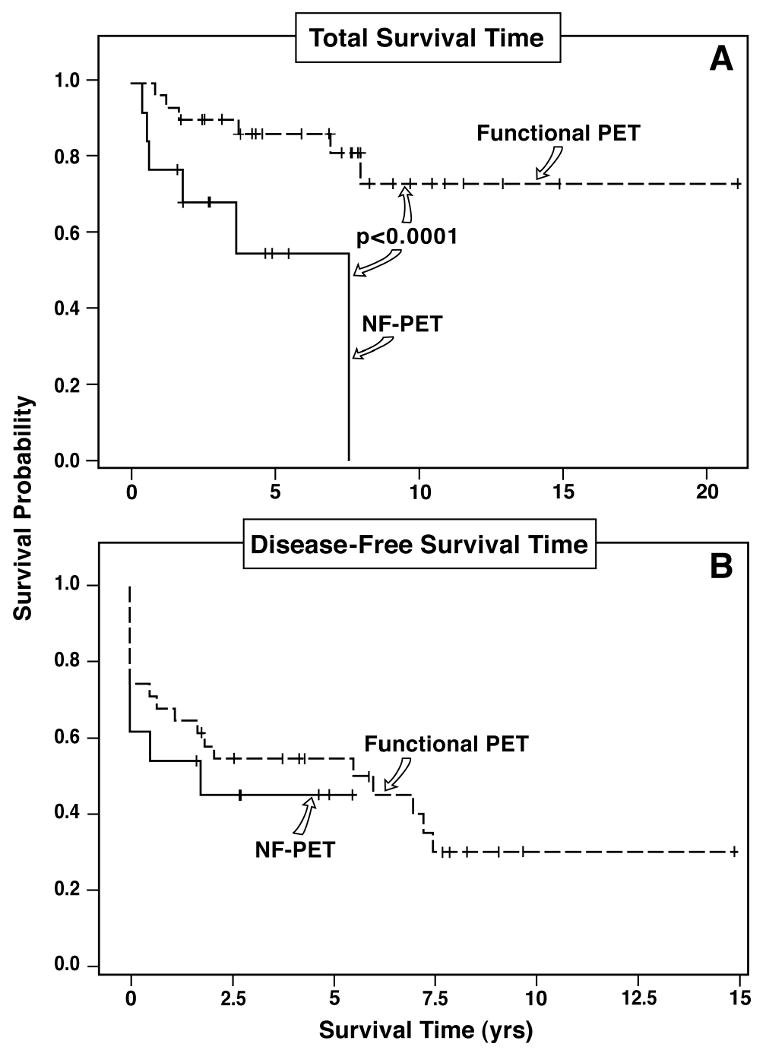
Results: Of 273 patients with PETs, 46 (17%) had preoperative computed tomography evidence of major vascular involvement. The mean size for the primary PET was 5.0 cm. The involved major vessel was as follows: portal vein (n = 20), superior mesenteric vein or superior mesenteric artery (n = 16), inferior vena cava (n = 4), splenic vein (n = 4), and heart (n = 2). Forty-two of 46 patients had a PET removed: 12 (27%) primary only, 30 (68%) with lymph nodes, and 18 (41%) with liver metastases. PETs were removed by either enucleation (n = 7) or resection (n = 35). Resections included distal or subtotal pancreatectomy in 23, Whipple in 10, and total in 2. Eighteen patients had concomitant liver resection: 10 wedge resection and 8 anatomic resections. Nine patients had vascular reconstruction: each had reconstruction of the superior mesenteric vein and portal vein, and 1 had concomitant reconstruction of the superior mesenteric artery. There were no deaths, but 12 patients had complications. Eighteen patients (41%) were immediately disease free, and 5 recurred with follow-up, leaving 13 (30%) disease-free long term. The 10-year overall survival was 60%. Functional tumors were associated with a better overall survival (P < .001), and liver metastases decreased overall survival (P < .001).
Conclusion: These findings suggest that surgical resection of PETs with vascular abutment/invasion and nodal or distant metastases is indicated.
Figures
Comment in
-
Especially dangerous and therefore anxious operations.Arch Surg. 2011 Jun;146(6):732-3. doi: 10.1001/archsurg.2011.110. Arch Surg. 2011. PMID: 21830340 No abstract available.
References
-
- Phan GQ, Yeo CJ, Hruban RH, Lillemoe KD, Pitt HA, Cameron JL. Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: review of 125 patients. J Gastrointest Surg. 1998 September;2(5):472–82. - PubMed
-
- Hochwald SN, Zee S, Conlon KC, et al. Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol. 2002 June 1;20(11):2633–42. - PubMed
-
- Jensen RT. Natural history of digestive endocrine tumors. In: Mignon M, Colombel JF, editors. Recent advances in pathophysiology and management of inflammatory bowel diseases and digestive endocrine tumors. Paris, France: John Libbey Eurotext Publishing Co.; 1999. pp. 192–219.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
