

Exercise training versus propranolol in the treatment of the postural orthostatic tachycardia syndrome
- PMID: 21690484
- PMCID: PMC3142863
- DOI: 10.1161/HYPERTENSIONAHA.111.172262
Exercise training versus propranolol in the treatment of the postural orthostatic tachycardia syndrome
Abstract
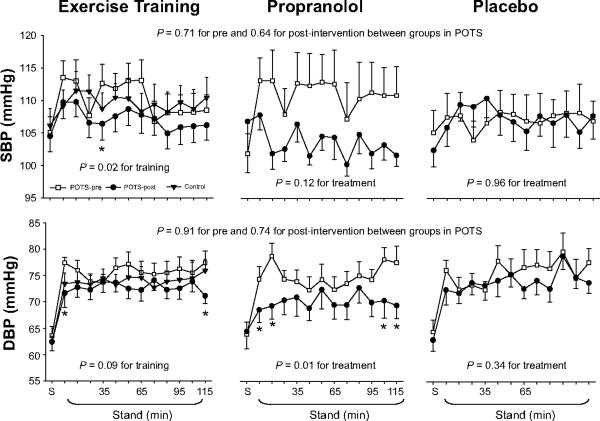
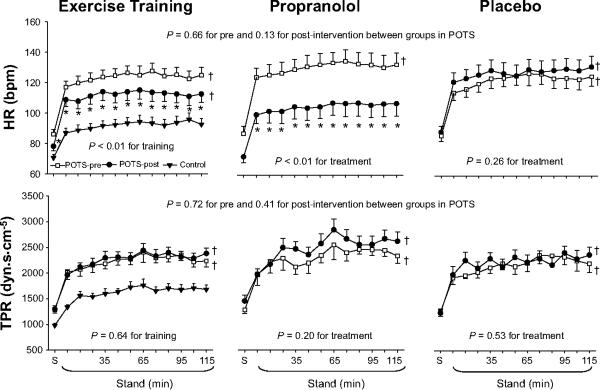
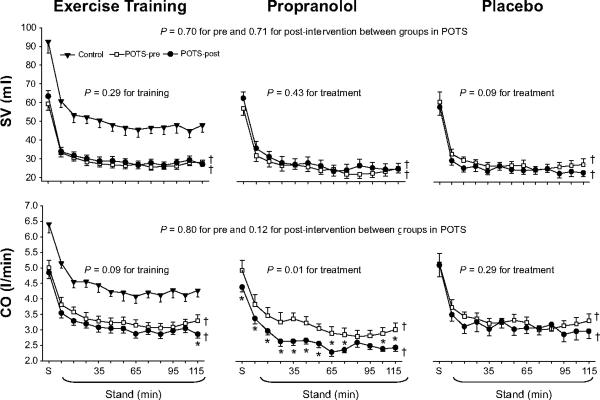
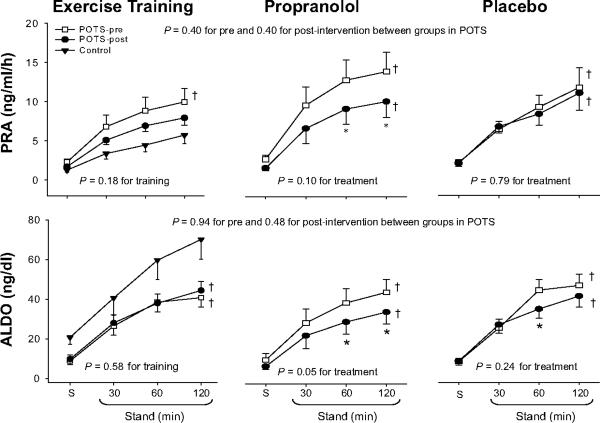
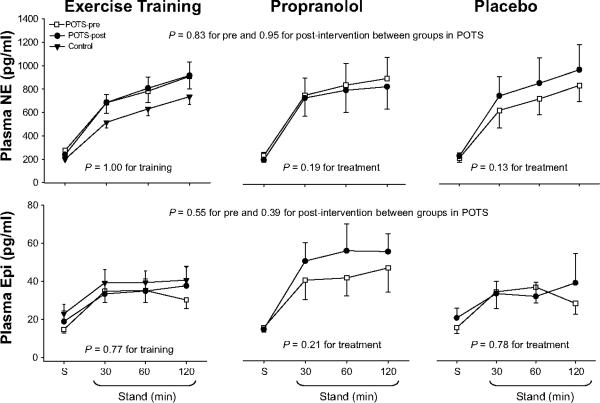
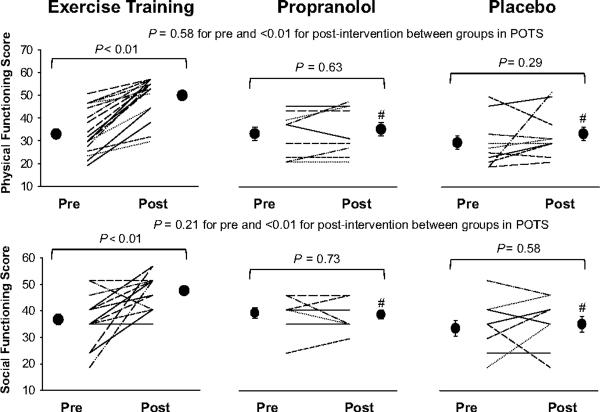
We have found recently that exercise training is effective in the treatment of the postural orthostatic tachycardia syndrome (POTS). Whether this nondrug treatment is superior to "standard" drug therapies, such as β-blockade, is unknown. We tested the hypothesis that exercise training but not β-blockade treatment improves symptoms, hemodynamics, and renal-adrenal responses in POTS patients. Nineteen patients (18 women and 1 man) completed a double-blind drug trial (propranolol or placebo) for 4 weeks, followed by 3 months of exercise training. Fifteen age-matched healthy individuals (14 women and 1 man) served as controls. A 2-hour standing test was performed before and after drug treatment and training. Hemodynamics, catecholamines, plasma renin activity, and aldosterone were measured supine and during 2-hour standing. We found that both propranolol and training significantly lowered standing heart rate. Standing cardiac output was lowered after propranolol treatment (P=0.01) but was minimally changed after training. The aldosterone:renin ratio during 2-hour standing remained unchanged after propranolol treatment (4.1±1.7 [SD] before versus 3.9±2.0 after; P=0.46) but modestly increased after training (5.2±2.9 versus 6.5±3.0; P=0.05). Plasma catecholamines were not affected by propranolol or training. Patient quality of life, assessed using the 36-item Short-Form Health Survey, was improved after training (physical functioning score 33±10 before versus 50±9 after; social functioning score 37±9 versus 48±6; both P<0.01) but not after propranolol treatment (34±10 versus 36±11, P=0.63; 39±7 versus 39±5, P=0.73). These results suggest that, for patients with POTS, exercise training is superior to propranolol at restoring upright hemodynamics, normalizing renal-adrenal responsiveness, and improving quality of life.
Figures
Comment in
-
Exercise training in Postural Orthostatic Tachycardia syndrome: blocking the urge to block β-receptors?Hypertension. 2011 Aug;58(2):136-7. doi: 10.1161/HYPERTENSIONAHA.111.173872. Epub 2011 Jun 20. Hypertension. 2011. PMID: 21690485 No abstract available.
References
-
- Rowell LB. Human Cardiovascular Control. Oxford University Press; New York, NY: 1993. Neural-humoral adjustments to orthostasis and long-term control; pp. 81–117.
-
- Raj SR, Biaggioni I, Yamhure PC, Black BK, Paranjape SY, Byrne DW, Robertson D. Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation. 2005;111:1574–1582. - PubMed
-
- Garland EM, Raj SR, Black BK, Harris PA, Robertson D. The hemodynamic and neurohumoral phenotype of postural tachycardia syndrome. Neurology. 2007;69:790–798. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
