

Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004
- PMID: 21690489
- PMCID: PMC3139992
- DOI: 10.1161/CIRCULATIONAHA.110.003954
Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004
Abstract
Background: Whether individuals with peripheral artery disease (PAD) identified by screening ankle-brachial index benefit from preventive therapies to reduce cardiovascular risk is unknown. We aimed to determine the number of US adults with PAD who are not receiving preventive therapies and whether treatment is associated with reduced mortality in PAD subjects without known cardiovascular disease.
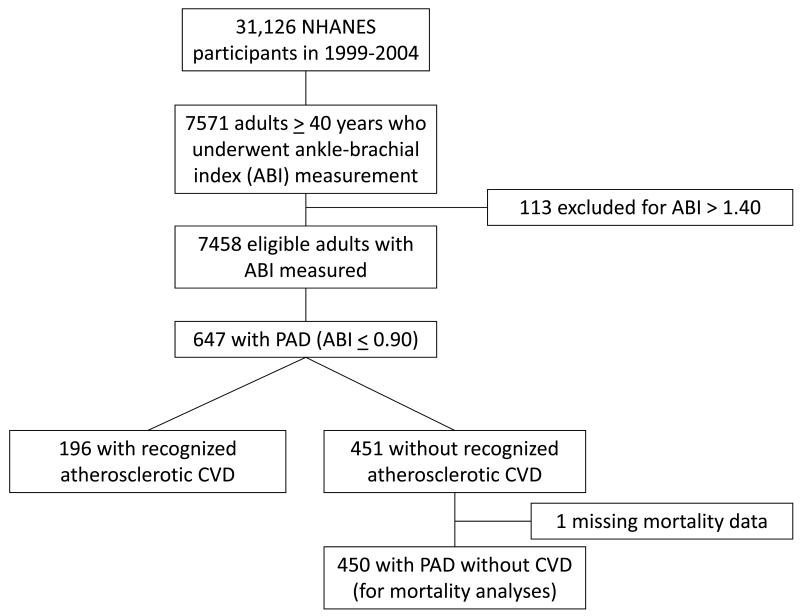
Methods and results: We analyzed data from the National Health and Nutrition Examination Survey (NHANES) 1999 to 2004 with mortality follow-up through December 31, 2006. We defined PAD as an ankle-brachial index ≤0.90. Of 7458 eligible participants ≥40 years, weighted PAD prevalence was 5.9±0.3% (mean±SE), corresponding to ≈7.1 million US adults with PAD. Statin use was reported in only 30.5±2.5%, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use in 24.9±1.9%, and aspirin use in 35.8±2.9%, corresponding to 5.0 million adults with PAD not taking statins, 5.4 million not taking angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, and 4.5 million not receiving aspirin. After adjustment for age, sex, and race/ethnicity, PAD was associated with all-cause mortality (hazard ratio, 2.4; 95% confidence interval, 1.9 to 2.9; P<0.0001). Even after exclusion of individuals with known cardiovascular disease, subjects with PAD had higher mortality rates (16.1±2.1%) than subjects without PAD or cardiovascular disease (4.1±0.3%), with an adjusted hazard ratio of 1.9 (95% confidence interval, 1.3 to 2.8; P=0.001). Among PAD subjects without cardiovascular disease, use of multiple preventive therapies was associated with 65% lower all-cause mortality (hazard ratio, 0.35; 95% confidence interval, 0.20 to 0.86; P=0.02).
Conclusions: Millions of US adults with PAD are not receiving secondary prevention therapies. Treatment with multiple therapies is associated with reduced all-cause mortality.
Conflict of interest statement
Figures
References
-
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, Rosenfield KA, Sacks D, Stanley JC, Taylor LM, Jr, White CJ, White J, White RA, Antman EM, Smith SC, Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113:e463–654. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) J Vasc Surg. 2007;45 S:S5–67. - PubMed
-
- Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, Krook SH, Hunninghake DB, Comerota AJ, Walsh ME, McDermott MM, Hiatt WR. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286:1317–1324. - PubMed
-
- Cacoub PP, Abola MT, Baumgartner I, Bhatt DL, Creager MA, Liau CS, Goto S, Rother J, Steg PG, Hirsch AT. Cardiovascular risk factor control and outcomes in peripheral artery disease patients in the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Atherosclerosis. 2009;204:e86–92. - PubMed
-
- Randomized trial of the effects of cholesterol-lowering with simvastatin on peripheral vascular and other major vascular outcomes in 20,536 people with peripheral arterial disease and other high-risk conditions. J Vasc Surg. 2007;45:645–654. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
