

Peripheral and central fat changes in subjects randomized to abacavir-lamivudine or tenofovir-emtricitabine with atazanavir-ritonavir or efavirenz: ACTG Study A5224s
- PMID: 21690627
- PMCID: PMC3165963
- DOI: 10.1093/cid/cir324
Peripheral and central fat changes in subjects randomized to abacavir-lamivudine or tenofovir-emtricitabine with atazanavir-ritonavir or efavirenz: ACTG Study A5224s
Abstract
Background: We compare the effect of 4 different antiretroviral regimens on limb and visceral fat.
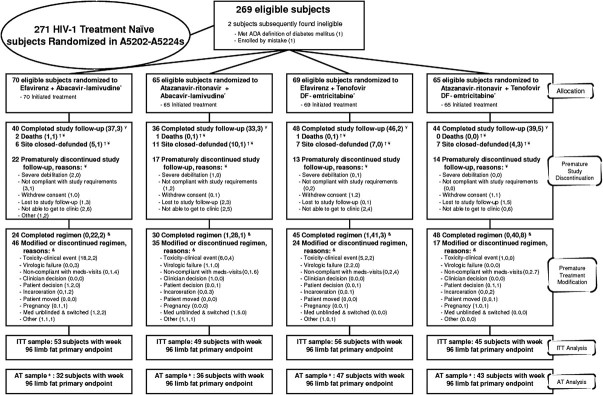
Methods: A5224s was a substudy of A5202, a trial of human immunodeficiency virus type 1 (HIV-1)-infected, treatment-naive subjects randomized to blinded abacavir-lamivudine (ABC-3TC) or tenofovir DF-emtricitabine (TDF-FTC) with open-label efavirenz (EFV) or atazanavir-ritonavir (ATV-r). The primary endpoint was the presence of lipoatrophy (≥ 10% loss of limb fat) at week 96 by intent-to-treat (ITT) analysis. Secondary endpoints included changes in limb and visceral fat. Statistical tests included linear regression, binomial, two-sample t test, and Fisher's exact test.
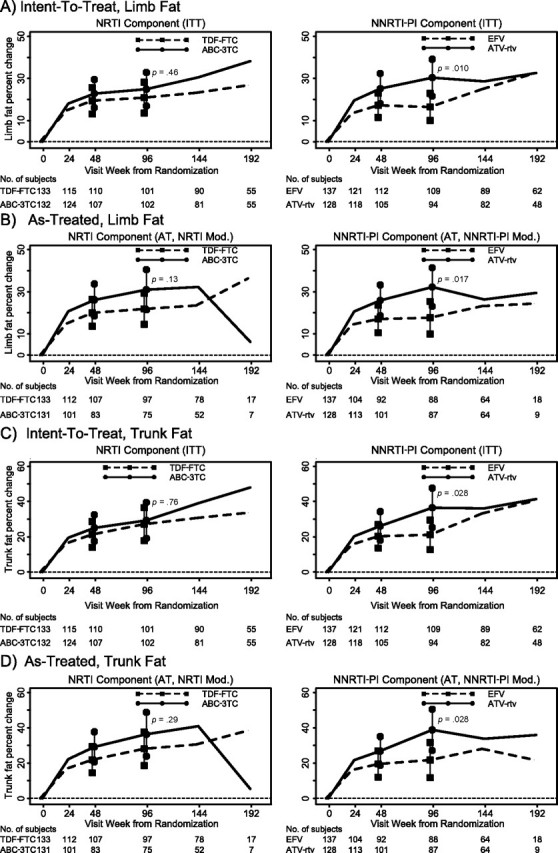
Results: A5224s enrolled 269 subjects; 85% were male, and 47% were white non-Hispanic. The subjects had a median baseline HIV-1 RNA level of 4.6 log(10) copies/mL, a median age of 38 years, a median CD4+ cell count of 233 cells/μL, median limb fat of 7.4 kg, median visceral adipose tissue (VAT) of 84.1 cm(2), and VAT: total adipose tissue (TAT) ratio of 0.31. At week 96, estimated prevalence of lipoatrophy (upper 95% confidence interval [CI]) was 18% (25%) for ABC-3TC and 15% (22%) for TDF-FTC (P = .70); this was not significantly less than the hypothesized 15% for both (P ≥ .55 for both). The secondary as-treated (AT) analysis showed similar results. At week 96, the estimated mean percentage change from baseline in VAT was higher for the ATV-r group than for the EFV group (26.6% vs 12.4%; P = .090 in ITT analysis and 30.0% vs 14.5%; P = .10 in AT analysis); however, the percentage change in VAT:TAT was similar by ITT and AT analysis (P ≥ .60 for both). Results were similar for absolute changes in VAT and VAT:TAT.
Conclusions: ABC-3TC- and TDF-FTC-based regimens increased limb and visceral fat at week 96, with a similar prevalence of lipoatrophy. Compared to the EFV group, subjects assigned to ATV-r had a trend towards higher mean percentage increase in VAT.
Clinical trials registration: NCT00118898.
Figures
References
-
- Walker UA, Bickel M, Lutke Volksbeck SI, et al. Evidence of nucleoside analogue reverse transcriptase inhibitor—associated genetic and structural defects of mitochondria in adipose tissue of HIV-infected patients. J Acquir Immune Defic Syndr. 2002;29:117–121. - PubMed
-
- Brinkman K, ter Hofstede HJ, Burger DM, Smeitink JA, Koopmans PP. Adverse effects of reverse transcriptase inhibitors: mitochondrial toxicity as common pathway. AIDS. 1998;12:1735–1744. - PubMed
-
- McComsey GA, Walker UA. Role of mitochondria in HIV lipoatrophy: insight into pathogenesis and potential therapies. Mitochondrion. 2004;4:111–118. - PubMed
-
- Cooper DA. Anthropometric and metabolic outcomes in a 48 week randomized, open-label study of three different combination antiretroviral regimens as initial therapy for HIV infection international workshop on Adverse Drug Reactions and Co-morbidities in HIV. Philadelphia, PA: 2009.
-
- Noor MA, Flint OP, Maa JF, Parker RA. Effects of atazanavir/ritonavir and lopinavir/ritonavir on glucose uptake and insulin sensitivity: demonstrable differences in vitro and clinically. AIDS. 2006;20:1813–1821. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 RR033176/RR/NCRR NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01 AI069424/AI/NIAID NIH HHS/United States
- AI065348/AI/NIAID NIH HHS/United States
- UM1 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069472/AI/NIAID NIH HHS/United States
- U01 AI68634/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- AI69501/AI/NIAID NIH HHS/United States
- U01 AI069501/AI/NIAID NIH HHS/United States
- AI0450008/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- AI069424/AI/NIAID NIH HHS/United States
- R01 AI065348/AI/NIAID NIH HHS/United States
- AI069472/AI/NIAID NIH HHS/United States
- AI38855/AI/NIAID NIH HHS/United States
- U01 AI069472/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
