

The collagen VI-related myopathies: muscle meets its matrix
- PMID: 21691338
- PMCID: PMC5210181
- DOI: 10.1038/nrneurol.2011.81
The collagen VI-related myopathies: muscle meets its matrix
Abstract
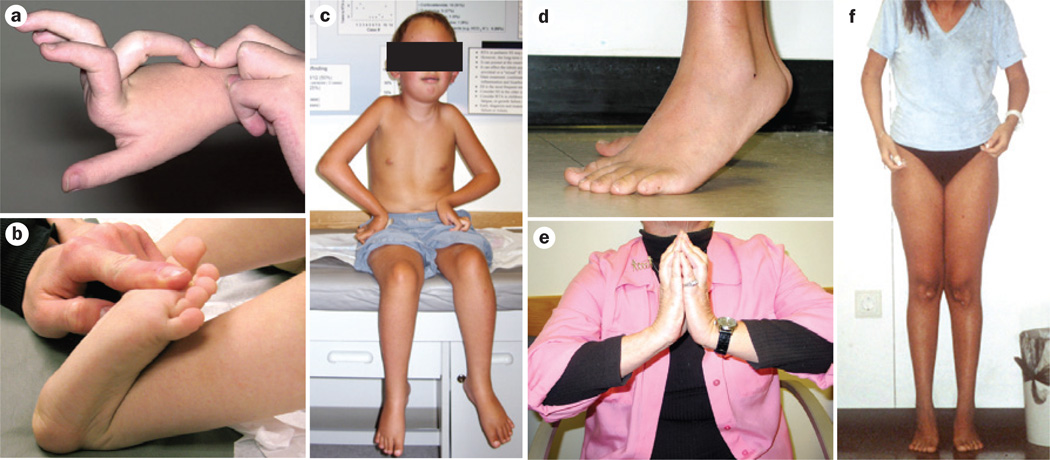
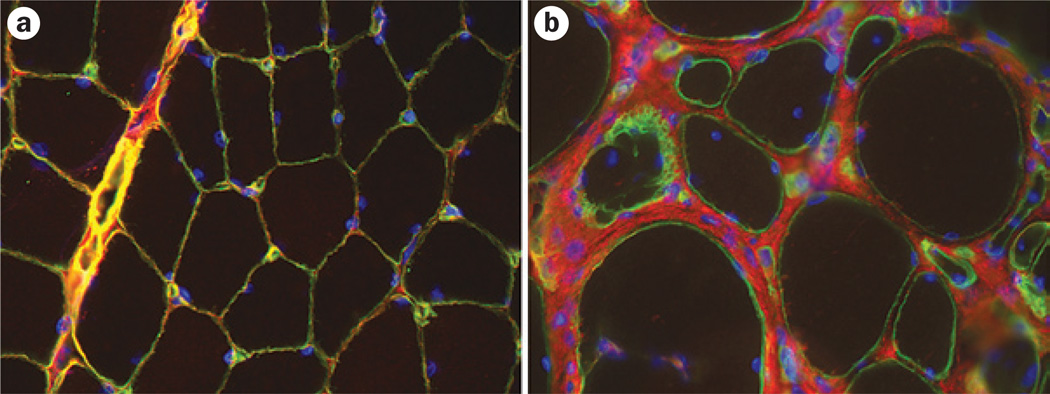
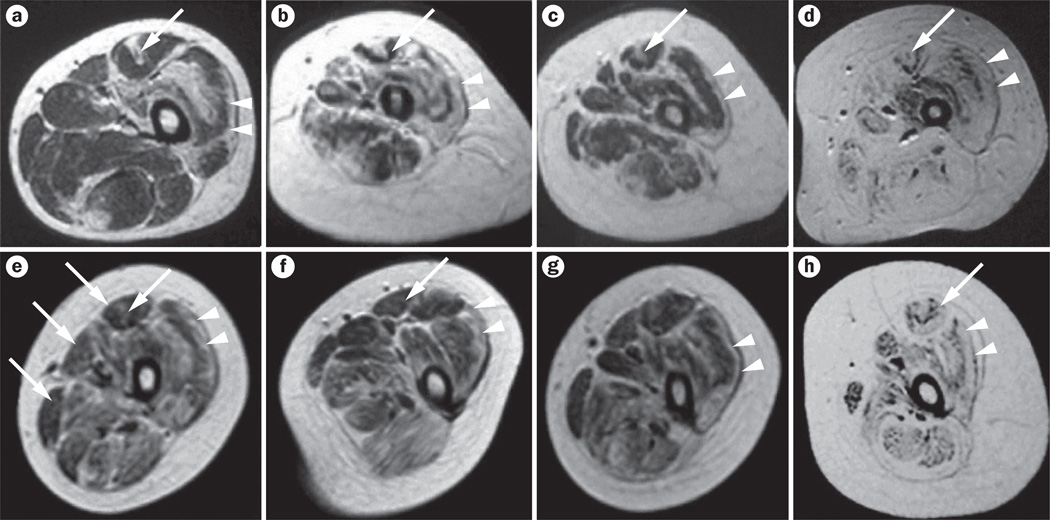
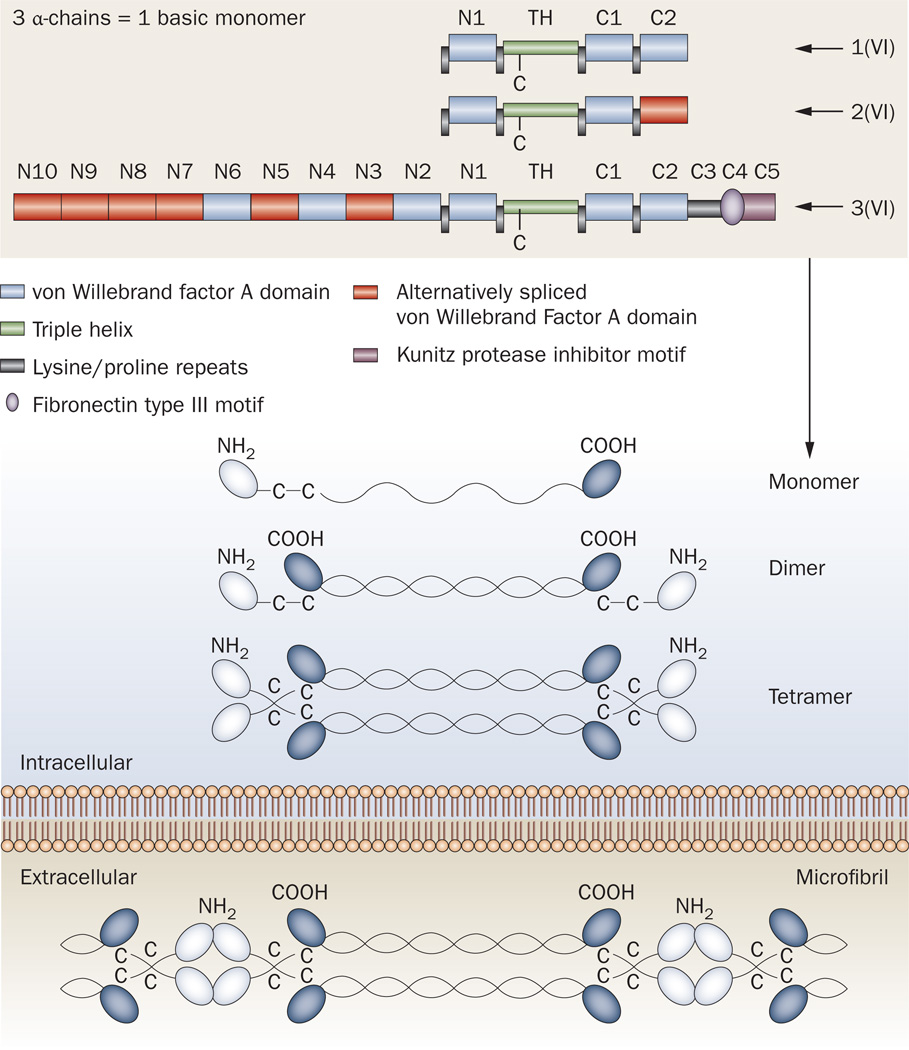
The collagen VI-related myopathy known as Ullrich congenital muscular dystrophy is an early-onset disease that combines substantial muscle weakness with striking joint laxity and progressive contractures. Patients might learn to walk in early childhood; however, this ability is subsequently lost, concomitant with the development of frequent nocturnal respiratory failure. Patients with intermediate phenotypes of collagen VI-related myopathy display a lesser degree of weakness and a longer period of ambulation than do individuals with Ullrich congenital muscular dystrophy, and the spectrum of disease finally encompasses mild Bethlem myopathy, in which ambulation persists into adulthood. Dominant and recessive autosomal mutations in the three major collagen VI genes-COL6A1, COL6A2, and COL6A3-can underlie this entire clinical spectrum, and result in deficient or dysfunctional microfibrillar collagen VI in the extracellular matrix of muscle and other connective tissues, such as skin and tendons. The potential effects on muscle include progressive dystrophic changes, fibrosis and evidence for increased apoptosis, which potentially open avenues for pharmacological intervention. Optimized respiratory management, including noninvasive nocturnal ventilation together with careful orthopedic management, are the current mainstays of treatment and have already led to a considerable improvement in life expectancy for children with Ullrich congenital muscular dystrophy.
Figures
References
-
- Okada M, et al. Primary collagen VI deficiency is the second most common congenital muscular dystrophy in Japan. Neurology. 2007;69:1035–1042. - PubMed
-
- Peat RA, et al. Diagnosis and etiology of congenital muscular dystrophy. Neurology. 2008;71:312–321. - PubMed
-
- Ullrich O. Congenital, atonic–sclerotic muscular dystrophy, an additional type of heredo-degenerative illness of the neuromuscular system [German] Z. Ges. Neurol. Psychiat. 1930;126:171–201.
-
- Ullrich O. Congenital atonic–sclerotic muscular dystrophy [German] Monatsschr. Kinderheilkd. 1930;47:502–510.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
