

Impact of changes in blood pressure during the treatment of acute decompensated heart failure on renal and clinical outcomes
- PMID: 21693504
- PMCID: PMC3143830
- DOI: 10.1093/eurjhf/hfr070
Impact of changes in blood pressure during the treatment of acute decompensated heart failure on renal and clinical outcomes
Abstract
Aims: One of the primary determinants of blood flow in regional vascular beds is perfusion pressure. Our aim was to investigate if reduction in blood pressure during the treatment of decompensated heart failure would be associated with worsening renal function (WRF). Our secondary aim was to evaluate the prognostic significance of this potentially treatment-induced form of WRF.
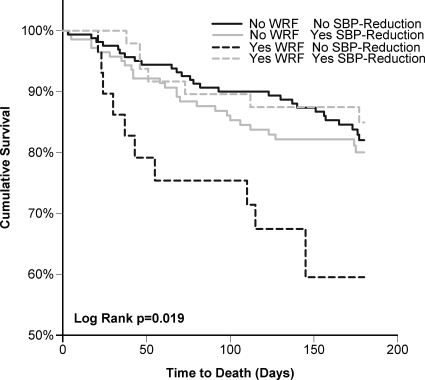
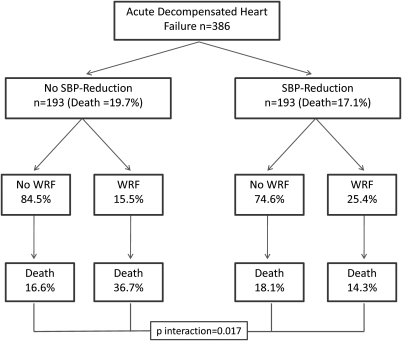
Methods and results: Subjects included in the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE) trial limited data were studied (386 patients). Reduction in systolic blood pressure (SBP) was greater in patients experiencing WRF (-10.3 ± 18.5 vs. -2.8 ± 16.0 mmHg, P < 0.001) with larger reductions associated with greater odds for WRF (odds ratio = 1.3 per 10 mmHg reduction, P < 0.001). Systolic blood pressure reduction (relative change > median) was associated with greater doses of in-hospital oral vasodilators (P ≤ 0.017), thiazide diuretic use (P = 0.035), and greater weight reduction (P = 0.023). In patients with SBP-reduction, WRF was not associated with worsened survival [adjusted hazard ratio (HR) = 0.76, P = 0.58]. However, in patients without SBP-reduction, WRF was strongly associated with increased mortality (adjusted HR = 5.3, P < 0.001, P interaction = 0.001).
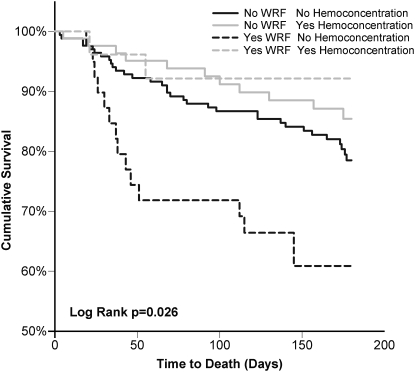
Conclusion: During the treatment of decompensated heart failure, significant blood pressure reduction is strongly associated with WRF. However, WRF that occurs in the setting of SBP-reduction is not associated with an adverse prognosis, whereas WRF in the absence of this provocation is strongly associated with increased mortality. These data suggest that WRF may represent the final common pathway of several mechanistically distinct processes, each with potentially different prognostic implications.
Figures
References
-
- Damman K, Navis G, Voors AA, Asselbergs FW, Smilde TD, Cleland JG, van Veldhuisen DJ, Hillege HL. Worsening renal function and prognosis in heart failure: systematic review and meta-analysis. J Card Fail. 2007;13:599–608. - PubMed
-
- Klein L, Massie BM, Leimberger JD, O'Connor CM, Pina IL, Adams KF, Jr., Califf RM, Gheorghiade M. Admission or changes in renal function during hospitalization for worsening heart failure predict postdischarge survival: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) Circ Heart Fail. 2008;1:25–33. - PubMed
-
- Nohria A, Hasselblad V, Stebbins A, Pauly DF, Fonarow GC, Shah M, Yancy CW, Califf RM, Stevenson LW, Hill JA. Cardiorenal interactions: insights from the ESCAPE trial. J Am Coll Cardiol. 2008;51:1268–1274. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
