

Diagnosis and management of iron deficiency anemia in the 21st century
- PMID: 21694802
- PMCID: PMC3105608
- DOI: 10.1177/1756283X11398736
Diagnosis and management of iron deficiency anemia in the 21st century
Abstract
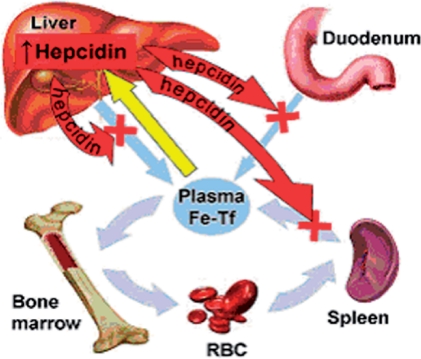
Iron deficiency is the single most prevalent nutritional deficiency worldwide. It accounts for anemia in 5% of American women and 2% of American men. The goal of this review article is to assist practitioners in understanding the physiology of iron metabolism and to aid in accurately diagnosing iron deficiency anemia. The current first line of therapy for patients with iron deficiency anemia is oral iron supplementation. Oral supplementation is cheap, safe, and effective at correcting iron deficiency anemia; however, it is not tolerated by some patients and in a subset of patients it is insufficient. Patients in whom the gastrointestinal blood loss exceeds the intestinal ability to absorb iron (e.g. intestinal angiodysplasia) may develop iron deficiency anemia refractory to oral iron supplementation. This population of patients proves to be the most challenging to manage. Historically, these patients have required numerous and frequent blood transfusions and suffer end-organ damage resultant from their refractory anemia. Intravenous iron supplementation fell out of favor secondary to the presence of infrequent but serious side effects. Newer and safer intravenous iron preparations are now available and are likely currently underutilized. This article discusses the possible use of intravenous iron supplementation in the management of patients with severe iron deficiency anemia and those who have failed oral iron supplementation.
Keywords: anemia; blood loss; intravenous iron; iron deficiency; therapy.
Figures
References
-
- Anderson G.J., Frazer D.M., McLaren G.D. (2009) Iron absorption and metabolism. Curr Opin Gastroenterol 25: 129–135 - PubMed
-
- Berger J., Dillon J.C. (2002) Control of iron deficiency in developing countries. Sante 12: 22–30 - PubMed
-
- Boley S.J., DiBiase A., Brandt L.J., Sammartano R.J. (1979) Lower intestinal bleeding in the elderly. Am J Surg 137: 57–64 - PubMed
-
- Byrnes V., Barrett S., Ryan E., Kelleher T., O’Keane C., Coughlan B., et al. (2002) Increased duodenal DMT-1 expression and unchanged HFE mRNA levels in HFE-associated hereditary hemochromatosis and iron deficiency. Blood Cells Mol Dis 29: 251–260 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
