

MRI pattern recognition in multiple sclerosis normal-appearing brain areas
- PMID: 21695053
- PMCID: PMC3117878
- DOI: 10.1371/journal.pone.0021138
MRI pattern recognition in multiple sclerosis normal-appearing brain areas
Abstract
Objective: Here, we use pattern-classification to investigate diagnostic information for multiple sclerosis (MS; relapsing-remitting type) in lesioned areas, areas of normal-appearing grey matter (NAGM), and normal-appearing white matter (NAWM) as measured by standard MR techniques.
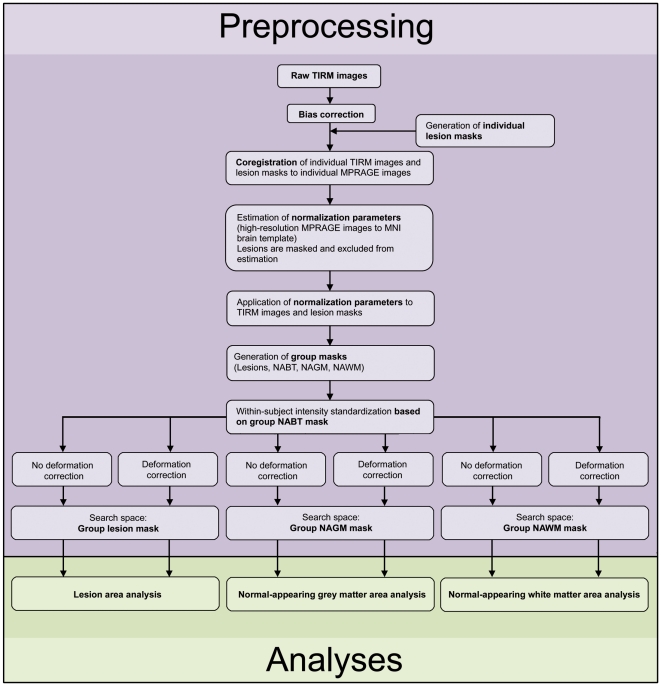
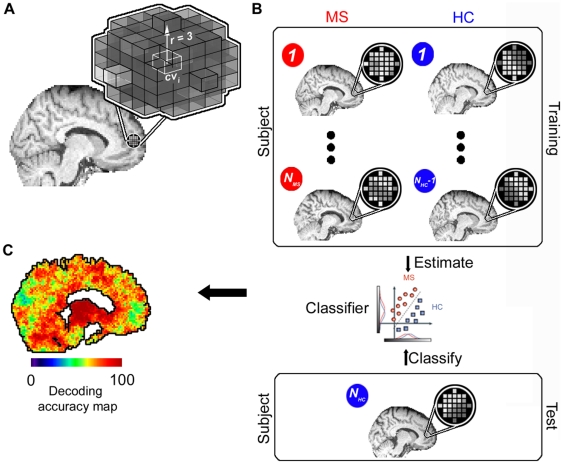
Methods: A lesion mapping was carried out by an experienced neurologist for Turbo Inversion Recovery Magnitude (TIRM) images of individual subjects. Combining this mapping with templates from a neuroanatomic atlas, the TIRM images were segmented into three areas of homogenous tissue types (Lesions, NAGM, and NAWM) after spatial standardization. For each area, a linear Support Vector Machine algorithm was used in multiple local classification analyses to determine the diagnostic accuracy in separating MS patients from healthy controls based on voxel tissue intensity patterns extracted from small spherical subregions of these larger areas. To control for covariates, we also excluded group-specific biases in deformation fields as a potential source of information.
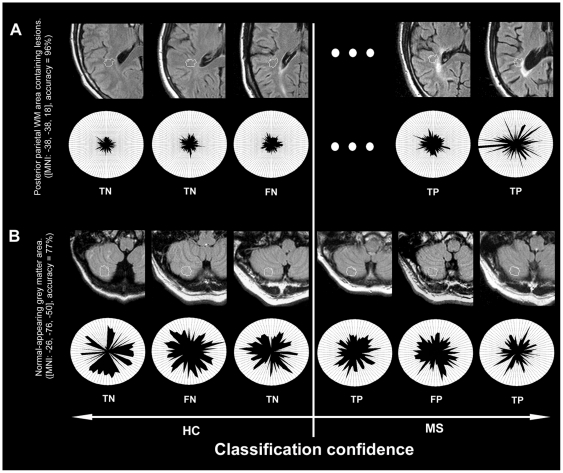
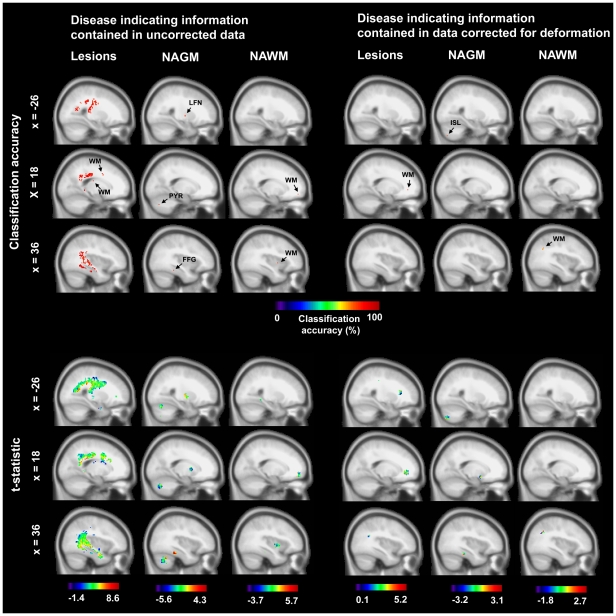
Results: Among regions containing lesions a posterior parietal WM area was maximally informative about the clinical status (96% accuracy, p<10(-13)). Cerebellar regions were maximally informative among NAGM areas (84% accuracy, p<10(-7)). A posterior brain region was maximally informative among NAWM areas (91% accuracy, p<10(-10)).
Interpretation: We identified regions indicating MS in lesioned, but also NAGM, and NAWM areas. This complements the current perception that standard MR techniques mainly capture macroscopic tissue variations due to focal lesion processes. Compared to current diagnostic guidelines for MS that define areas of diagnostic information with moderate spatial specificity, we identified hotspots of MS associated tissue alterations with high specificity defined on a millimeter scale.
Conflict of interest statement
Figures
References
-
- McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol. 2001;50:121–127. - PubMed
-
- Polman CH, Wolinsky JS, Reingold SC. Multiple sclerosis diagnostic criteria: three years later. Mult Scler. 2005;11:5–12. - PubMed
-
- Montalban X, Tintoré M, Swanton J, Barkhof F, Fazekas F, et al. MRI criteria for MS in patients with clinically isolated syndromes. Neurology. 2010;74:427–434. - PubMed
-
- Chard DT, Griffin CM, Rashid W, Davies GR, Altmann DR, et al. Progressive grey matter atrophy in clinically early relapsing-remitting multiple sclerosis. Mult Scler. 2004;10:387–391. - PubMed
-
- Valsasina P, Benedetti B, Rovaris M, Sormani MP, Comi G, et al. Evidence for progressive gray matter loss in patients with relapsingremitting MS. Neurology. 2005;65:1126–1128. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
