

Epidemiology of classical Hodgkin lymphoma and its association with Epstein Barr virus in Northern China
- PMID: 21695175
- PMCID: PMC3112231
- DOI: 10.1371/journal.pone.0021152
Epidemiology of classical Hodgkin lymphoma and its association with Epstein Barr virus in Northern China
Abstract
Background: The incidence of classical Hodgkin lymphoma (cHL) and its association with Epstein-Barr virus (EBV) varies significantly with age, sex, ethnicity and geographic location. This is the first report on epidemiological features of cHL patients from Northern regions of China. These features are compared to data from a previously published Dutch cHL population.
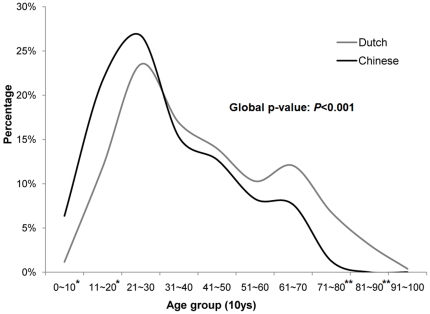
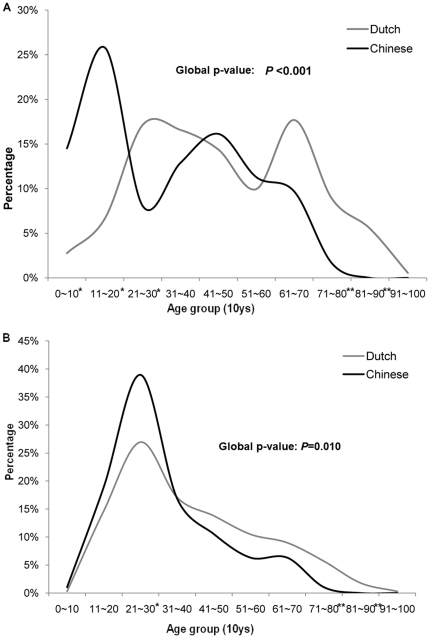
Methodology/principal findings: 157 cHL patients diagnosed between 1997 and 2008 in the North of China were included after histopathological re-evaluation. The Dutch population-based cohort consisted of 515 cHL patients diagnosed between 1987 and 2000. EBV status was determined by in situ hybridization of EBV- encoded small RNAs. In the Chinese population, tumor cells of 39% of the cHL patients were EBV+ and this was significantly associated with male sex, mixed cellularity subtype and young age (<20 y). The median age of the Chinese patients was 9 years younger than that of the Dutch patients (28 y vs. 37 y). In addition, the age distribution between the two populations was strikingly different in both the EBV+ subgroups (p<0.001) and the EBV- subgroups (p = 0.01). The mixed cellularity subtype was almost 3x more frequent amongst the Chinese (p<0.001).
Conclusion/significance: CHL patients from Northern regions of China show a distinctive age distribution pattern with a striking incidence peak of EBV+ mixed cellularity cases among children and adolescents and another high incidence peak of EBV- nodular sclerosis cases in young adults. In comparison to Dutch cHL patients there are pronounced differences in age distribution, subtype and EBV status, presumably caused by complex gene-environmental interactions.
Conflict of interest statement
Figures
References
-
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, et al. Lyon: IARC Press; 2008. WHO Classification of Tumors: Pathology and Genetics of Tumors of Haematopoietic and Lymphoid Tissues. pp. 321–334.
-
- Jarrett AF, Armstrong AA, Alexander E. Epidemiology of EBV and Hodgkin's lymphoma. Ann Oncol. 1996;7(Suppl 4):5–10. - PubMed
-
- Cartwright RA, Watkins G. Epidemiology of Hodgkin's disease: a review. Hematol Oncol. 2004;22:11–26. - PubMed
-
- Glaser SL, Hsu JL. Hodgkin's disease in Asians: incidence patterns and risk factors in population-based data. Leuk Res. 2002;26:261–269. - PubMed
-
- Au WY, Gascoyne RD, Gallagher RE, Le N, Klasa RD, et al. Hodgkin's lymphoma in Chinese migrants to British Columbia: a 25-year survey. Ann Oncol. 2004;15:626–630. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
