

Surgical management of vesicoureteral reflux in children
- PMID: 21695451
- PMCID: PMC3288369
- DOI: 10.1007/s00467-011-1933-7
Surgical management of vesicoureteral reflux in children
Abstract
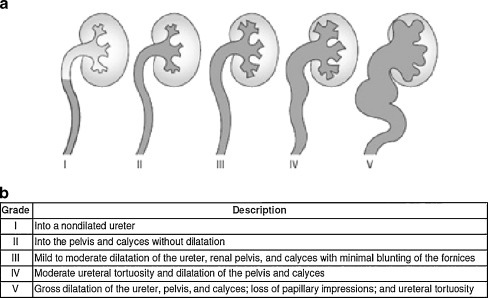
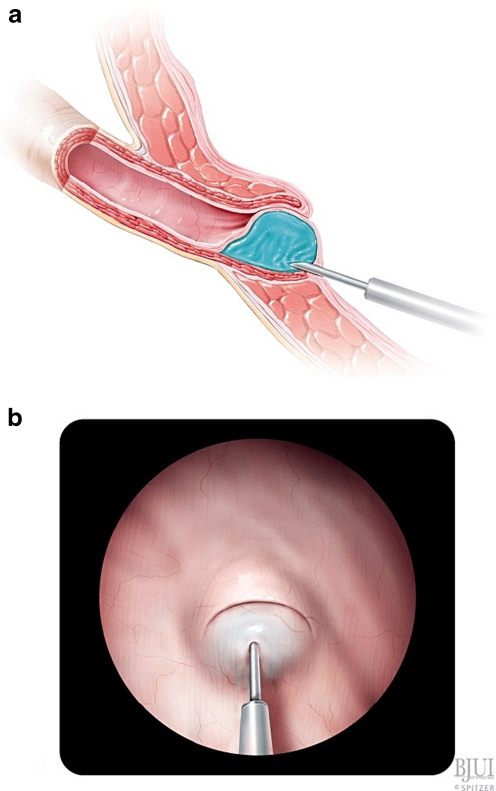
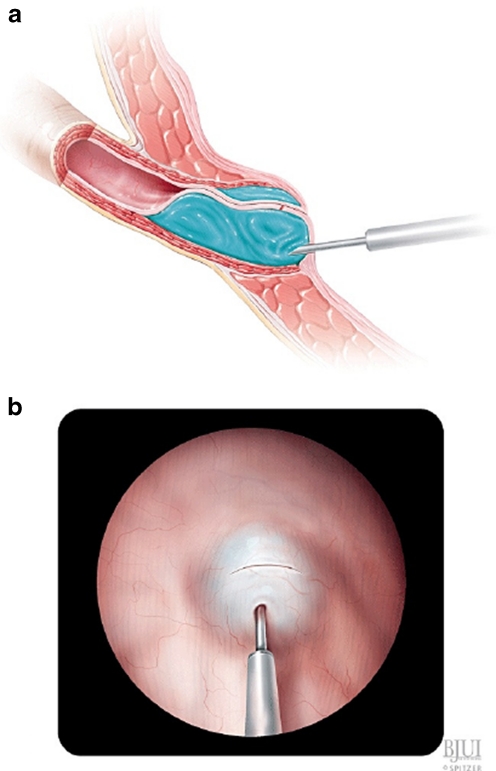
Vesicoureteral reflux (VUR) is the most common uropathy affecting children. Compared to children without VUR, those with VUR have a higher rate of pyelonephritis and renal scarring following urinary tract infection (UTI). Options for treatment include observation with or without antibiotic prophylaxis and surgical repair. Surgical intervention may be necessary in patients with persistent reflux, renal scarring, and recurrent or breakthrough febrile UTI. Both open and endoscopic approaches to reflux correction are successful and reduce the occurrence of febrile UTI. Estimated success rates of open and endoscopic reflux correction are 98.1% (95% CI 95.1, 99.1) and 83.0% (95% CI 69.1, 91.4), respectively. Factors that affect the success of endoscopic injection include pre-operative reflux grade and presence of functional or anatomic bladder abnormalities including voiding dysfunction and duplicated collecting systems. Few studies have evaluated the long-term outcomes of endoscopic injection, and with variable results. In patients treated endoscopically, recurrent febrile UTI occurred in 0-21%, new renal damage in 9-12%, and recurrent reflux in 17-47.6% of treated ureters with at least 1 year follow-up. These studies highlight the need for standardized outcome reporting and longer follow-up after endoscopic treatment.
Figures
References
-
- Bailey RR (1979) Vesicoureteral reflux in healthy infants and children. Reflux Nephropathy 59–61
-
- Skoog SJ, Peters CA, Arant BS, Jr, Copp HL, Elder JS, Hudson RG, Khoury AE, Lorenzo AJ, Pohl HG, Shapiro E, Snodgrass WT, Diaz M. Pediatric vesicoureteral reflux guideline panel summary report: clinical practice guidelines for screening siblings of children with vesicoureteral reflux and neonates/infants with prenatal hydronephrosis. J Urol. 2010;184(3):1145–1151. doi: 10.1016/j.juro.2010.05.066. - DOI - PubMed
-
- Zerin JM, Ritchey ML, Chang AC. Incidental vesicoureteral reflux in neonates with antenatally detected hydronephrosis and other renal abnormalities. Radiol. 1993;187:157–160. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
