

Field trial of three different Plasmodium vivax-detecting rapid diagnostic tests with and without evaporative cool box storage in Afghanistan
- PMID: 21696587
- PMCID: PMC3141591
- DOI: 10.1186/1475-2875-10-169
Field trial of three different Plasmodium vivax-detecting rapid diagnostic tests with and without evaporative cool box storage in Afghanistan
Abstract
Background: Accurate parasitological diagnosis of malaria is essential for targeting treatment where more than one species coexist. In this study, three rapid diagnostic tests (RDTs) (AccessBio CareStart (CSPfPan), CareStart PfPv (CSPfPv) and Standard Diagnostics Bioline (SDBPfPv)) were evaluated for their ability to detect natural Plasmodium vivax infections in a basic clinic setting. The potential for locally made evaporative cooling boxes (ECB) to protect the tests from heat damage in high summer temperatures was also investigated.
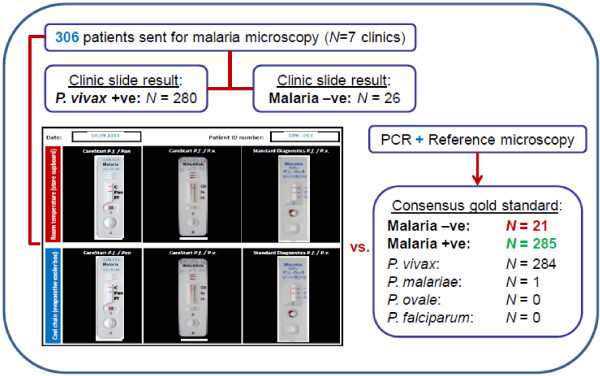
Methods: Venous blood was drawn from P. vivax positive patients in Jalalabad, Afghanistan and tested against a panel of six RDTs. The panel comprised two of each test type; one group was stored at room temperature and the other in an ECB. RDT results were evaluated against a consensus gold standard based on two double-read reference slides and PCR. The sensitivity, specificity and a measure of global performance for each test were determined and stratified by parasitaemia level and storage condition.
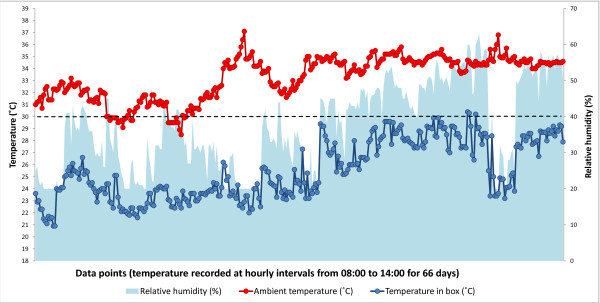
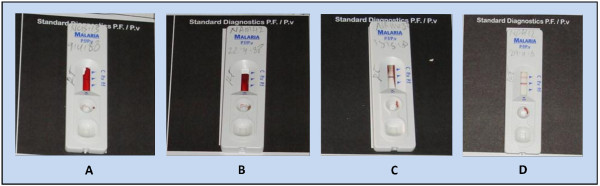
Results: In total, 306 patients were recruited, of which 284 were positive for P. vivax, one for Plasmodium malariae and none for Plasmodium falciparum; 21 were negative. All three RDTs were specific for malaria. The sensitivity and global performance index for each test were as follows: CSPfPan [98.6%, 95.1%], CSPfPv [91.9%, 90.5%] and SDBPfPv [96.5%, 82.9%], respectively. CSPfPv was 16% less sensitive to a parasitaemia below 5,000/μL. Room temperature storage of SDBPfPv led to a high proportion of invalid results (17%), which reduced to 10% in the ECB. Throughout the testing period, the ECB maintained ~8°C reduction over ambient temperatures and never exceeded 30°C.
Conclusions: Of the three RDTs, the CSPfPan test was the most consistent and reliable, rendering it appropriate for this P. vivax predominant region. The CSPfPv test proved unsuitable owing to its reduced sensitivity at a parasitaemia below 5,000/μL (affecting 43% of study samples). Although the SDBPfPv device was more sensitive than the CSPfPv test, its invalid rate was unacceptably high. ECB storage reduced the proportion of invalid results for the SDBPfPv test, but surprisingly had no impact on RDT sensitivity at low parasitaemia.
Figures

References
-
- World Health Organization. Guidelines for the treatment of malaria. 2. WHO Geneva; 2010. - PubMed
-
- Salwa ME, Abd EKA, Babiker A, Hayder A, Diagn MID. Malaria overdiagnosis and burden of malaria misdiagnosis in the suburbs of central Sudan: special emphasis on artemisinin-based combination therapy era. Diagn Microbiol Infect Dis. 2009;64:20–26. doi: 10.1016/j.diagmicrobio.2009.01.029. - DOI - PubMed
-
- Nicastri E, Bevilacqua N, Schepisi MS, Paglia MG, Meschi S, Ame SM, Mohamed JA, Mangi S, Fumakule R, Di Caro A. Accuracy of malaria diagnosis by microscopy, rapid diagnostic test, and PCR methods and evidence of antimalarial overprescription in non-severe febrile patients in two Tanzanian hospitals. Am J Trop Med Hyg. 2009;80:712–717. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
