

Adult presentation of PHACES syndrome
- PMID: 21696650
- PMCID: PMC3287263
- DOI: 10.1177/159101991101700201
Adult presentation of PHACES syndrome
Abstract
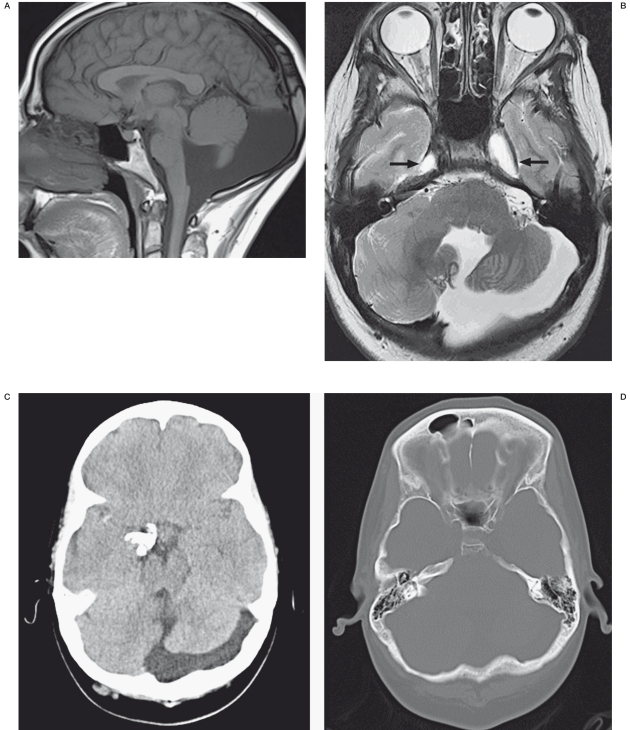
A significant percentage of children with hemangiomas may have PHACES syndrome which refers to the association of posterior fossa malformations, facial hemangiomas, arterial cerebrovascular abnormalities, cardiovascular anomalies, eye abnormalities and ventral defects like sternal clefting or supraumbilical raphe. A variety of factors have led to under diagnosis of PHACES syndrome in the past including lack of awareness and limited imaging modalities. Also, patients with PHACES syndrome with arterial cerebrovascular abnormalities can present with acute ischemic stroke. However, these patients usually present before one year of age. We describe a 29-year-old woman with no history of cerebrovascular disease who initially presented with symptoms of a stroke and was subsequently diagnosed to have PHACES syndrome exhibiting an array of multiple unusual imaging findings. We also discuss the current literature and recommendations about PHACES syndrome.
Figures






Similar articles
-
PHACES Syndrome and Associated Anomalies: Risk Associated With Small and Large Facial Hemangiomas.AJR Am J Roentgenol. 2021 Aug;217(2):507-514. doi: 10.2214/AJR.20.23488. Epub 2021 May 26. AJR Am J Roentgenol. 2021. PMID: 34036811
-
A unique case of PHACES syndrome confirming the assumption that PHACES syndrome and the sternal malformation-vascular dysplasia association are part of the same spectrum of malformations.Clin Dysmorphol. 2005 Oct;14(4):203-206. Clin Dysmorphol. 2005. PMID: 16155423
-
Ocular and systemic manifestations of PHACES (Posterior fossa malformations, Hemangiomas, Arterial anomalies, Cardiac defects and coarctation of the Aorta, Eye abnormalities, and Sternal abnormalities or ventral developmental defects) syndrome.J AAPOS. 2005 Apr;9(2):169-73. doi: 10.1016/j.jaapos.2004.08.012. J AAPOS. 2005. PMID: 15838446
-
PHACES syndrome associated with carcinoid endobronchial tumor.Pediatr Radiol. 2014 May;44(5):621-4. doi: 10.1007/s00247-013-2820-0. Epub 2013 Dec 13. Pediatr Radiol. 2014. PMID: 24337788 Review.
-
PHACE(S) syndrome.Handb Clin Neurol. 2015;132:169-83. doi: 10.1016/B978-0-444-62702-5.00012-3. Handb Clin Neurol. 2015. PMID: 26564079 Review.
Cited by
-
PHACES syndrome: Diode laser photocoagulation of intraoral hemangiomas in six young patients.Int J Surg Case Rep. 2015;11:124-128. doi: 10.1016/j.ijscr.2015.03.045. Epub 2015 Mar 27. Int J Surg Case Rep. 2015. PMID: 25974260 Free PMC article.
-
Localized Marked Elongation of the Distal Internal Carotid Artery with or without PHACE Syndrome: Segmental Dolichoectasia of the Distal Internal Carotid Artery.AJNR Am J Neuroradiol. 2018 May;39(5):817-823. doi: 10.3174/ajnr.A5573. Epub 2018 Mar 15. AJNR Am J Neuroradiol. 2018. PMID: 29545249 Free PMC article.
-
Concomitant carotid aplasia and basilar artery occlusion in a child with PHACES syndrome.BMJ Case Rep. 2017 Aug 16;2017:bcr2017221055. doi: 10.1136/bcr-2017-221055. BMJ Case Rep. 2017. PMID: 28814594 Free PMC article.
-
Correction of aortic coarctation in a girl with severe PHACE syndrome.J Cardiothorac Surg. 2014 Oct 14;9:169. doi: 10.1186/s13019-014-0169-6. J Cardiothorac Surg. 2014. PMID: 25312304 Free PMC article.
-
Phaces syndrome with intraoral and perioral hemangiomas: a different approach with Diode Laser.Ann Stomatol (Roma). 2013 Oct 24;4(Suppl 2):42-3. eCollection 2013. Ann Stomatol (Roma). 2013. PMID: 24353816 Free PMC article. No abstract available.
References
-
- Frieden IJ, Reese V, Cohen D. PHACE syndrome. The association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol. 1996;132:307–311. - PubMed
-
- Bhattacharya JJ, Luo CB, Alvarez H, et al. PHACES syndrome: a review of eight previously unreported cases with late arterial occlusions. Neuroradiology. 2004;46:227–233. - PubMed
-
- Metry D, Heyer G, Hess C, et al. Consensus statement on diagnostic criteria for PHACE syndrome. Pediatrics. 2009;124:1447–1456. - PubMed
-
- Heyer GL, Millar WS, Ghatan S, et al. The neurologic aspects of PHACE: case report and review of the literature. Pediatr Neurol. 2006;35:419–424. - PubMed
-
- Haggstrom AN, Garzon MC, Baselga E, et al. Risk for PHACE syndrome in infants with large facial hemangiomas. Pediatrics. 2010;126:e418–426. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
