

High-resolution CT of complications of idiopathic fibrotic lung disease
- PMID: 21697412
- PMCID: PMC3473493
- DOI: 10.1259/bjr/65090500
High-resolution CT of complications of idiopathic fibrotic lung disease
Abstract
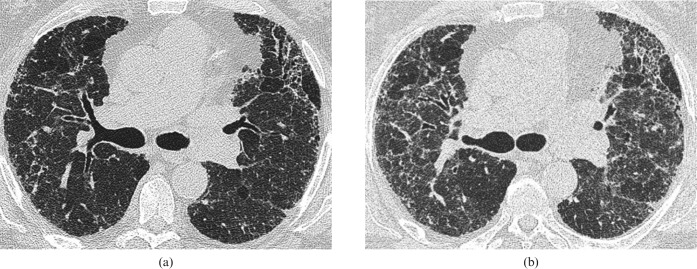
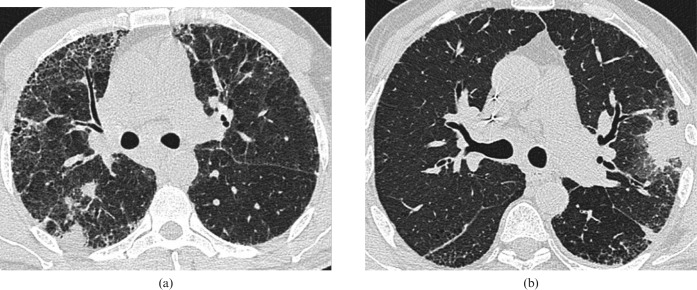
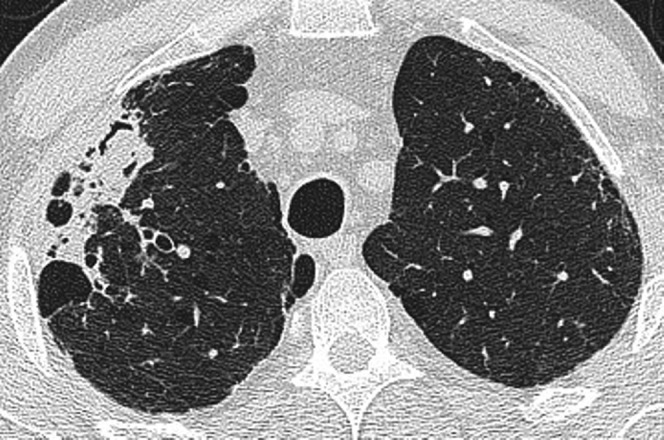
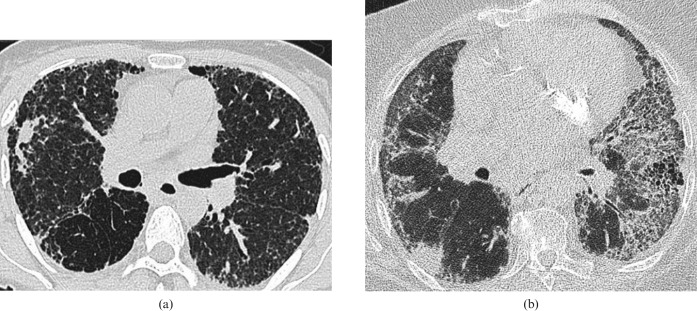
Idiopathic pulmonary fibrosis (IPF) has a more variable clinical course than has been traditionally recognised. Many patients will remain stable over time while others experience relatively rapid deterioration. The prognosis and clinical course of patients with other fibrosing lung diseases is also variable. A number of conditions may complicate the clinical course of the idiopathic fibrosing lung diseases, which results in morbidity and mortality, but also represents potentially treatable causes of worsening symptoms. Infection and malignancy have a long-recognised association with IPF while other conditions, particularly pulmonary hypertension and acute exacerbation of IPF, are being increasingly recognised in this patient population. Many of these patients have serial high-resolution CT (HRCT) examinations that may demonstrate one or more of these supervening conditions. In this article we review the more common conditions that may complicate the course of idiopathic fibrosing lung disease with an emphasis on the HRCT appearance, which the reporting radiologist should be aware of.
Figures

Similar articles
-
Imaging Review of the Lung Parenchymal Complications in Patients with IPF.Medicina (Kaunas). 2019 Sep 20;55(10):613. doi: 10.3390/medicina55100613. Medicina (Kaunas). 2019. PMID: 31547107 Free PMC article. Review.
-
Idiopathic Pulmonary Fibrosis.J Thorac Imaging. 2016 May;31(3):127-39. doi: 10.1097/RTI.0000000000000204. J Thorac Imaging. 2016. PMID: 27043425 Review.
-
Acute Exacerbation of Idiopathic Pulmonary Fibrosis.Medicina (Kaunas). 2019 Mar 16;55(3):70. doi: 10.3390/medicina55030070. Medicina (Kaunas). 2019. PMID: 30884853 Free PMC article. Review.
-
Assessment of Lung Cancer Development in Idiopathic Pulmonary Fibrosis Patients Using Quantitative High-Resolution Computed Tomography: A Retrospective Analysis.J Thorac Imaging. 2020 Mar;35(2):115-122. doi: 10.1097/RTI.0000000000000468. J Thorac Imaging. 2020. PMID: 31913257
-
Serial changes and prognostic implications of CT findings in combined pulmonary fibrosis and emphysema: comparison with fibrotic idiopathic interstitial pneumonias alone.Acta Radiol. 2017 May;58(5):550-557. doi: 10.1177/0284185116664227. Epub 2016 Sep 30. Acta Radiol. 2017. PMID: 27565631
Cited by
-
Characteristics and evaluation of acute exacerbations in chronic interstitial lung diseases.Respir Med. 2021 Jul;183:106400. doi: 10.1016/j.rmed.2021.106400. Epub 2021 Apr 26. Respir Med. 2021. PMID: 33957435 Free PMC article. Review.
-
Imaging Review of the Lung Parenchymal Complications in Patients with IPF.Medicina (Kaunas). 2019 Sep 20;55(10):613. doi: 10.3390/medicina55100613. Medicina (Kaunas). 2019. PMID: 31547107 Free PMC article. Review.
-
Diagnosis and Treatment of Lung Cancer in the Setting of Interstitial Lung Disease.Radiol Clin North Am. 2022 Nov;60(6):993-1002. doi: 10.1016/j.rcl.2022.06.010. Epub 2022 Sep 3. Radiol Clin North Am. 2022. PMID: 36202484 Free PMC article. Review.
-
Serum analysis of coagulation factors in IPF and NSIP.Inflammation. 2014 Feb;37(1):10-6. doi: 10.1007/s10753-013-9706-z. Inflammation. 2014. PMID: 23912648
-
Complications in Idiopathic Pulmonary Fibrosis: Focus on Their Clinical and Radiological Features.Diagnostics (Basel). 2020 Jul 3;10(7):450. doi: 10.3390/diagnostics10070450. Diagnostics (Basel). 2020. PMID: 32635390 Free PMC article.
References
-
- American Thoracic Society/European Respiratory Society International multidisciplinary consensus classification of idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2002;165:277–304 - PubMed
-
- Bjoraker JA, Ryu JH, Edwin MK, Myers JL, Tazelaar HD, Schroeder DR, et al. Prognostic significance of histopathologic subsets in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1998;157:199–203 - PubMed
-
- Hubbard R, Johnston I, Britton J. Survival in patients with cryptogenic fibrosis alveolitis: a population-based cohort study. Chest 1998;113:396–400 - PubMed
-
- Nicholson AG, Colby TV, du Bois RM, Hansell DM, Wells AU. The prognostic significance of the histologic pattern of interstitial pneumonia in patients presenting with the clinical entity of cryptogenic fibrosing alveolitis. Am J Respir Crit Care Med 2000;162:2213–17 - PubMed
