

Geographic disparities in chronic obstructive pulmonary disease (COPD) hospitalization among Medicare beneficiaries in the United States
- PMID: 21697996
- PMCID: PMC3119107
- DOI: 10.2147/COPD.S19945
Geographic disparities in chronic obstructive pulmonary disease (COPD) hospitalization among Medicare beneficiaries in the United States
Abstract
Background: Hospitalizations for persons with chronic obstructive pulmonary disease (COPD) result in significant health care resource use and excess expenditures. Despite well-documented sociodemographic disparities in COPD outcomes, no study has characterized geographic variations in COPD hospitalization across the US.
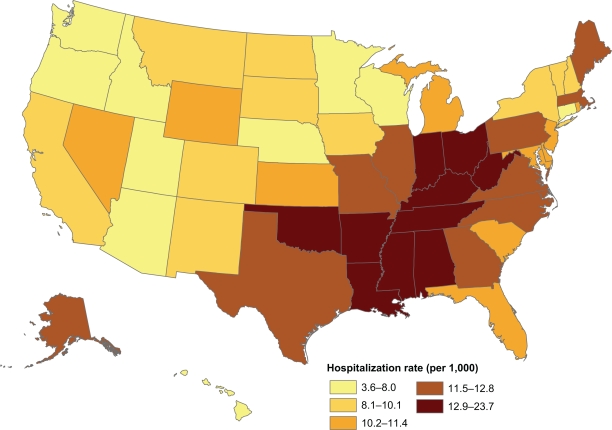
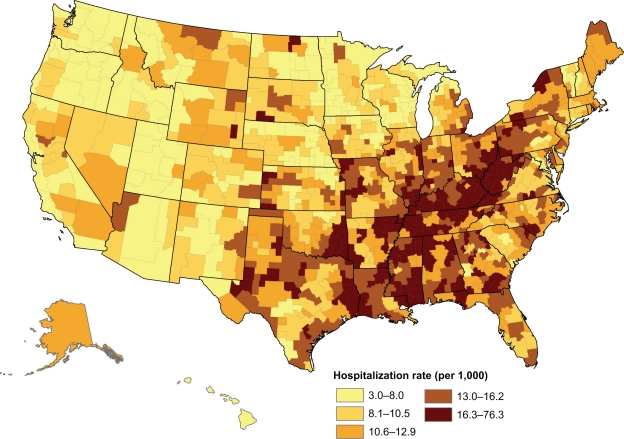
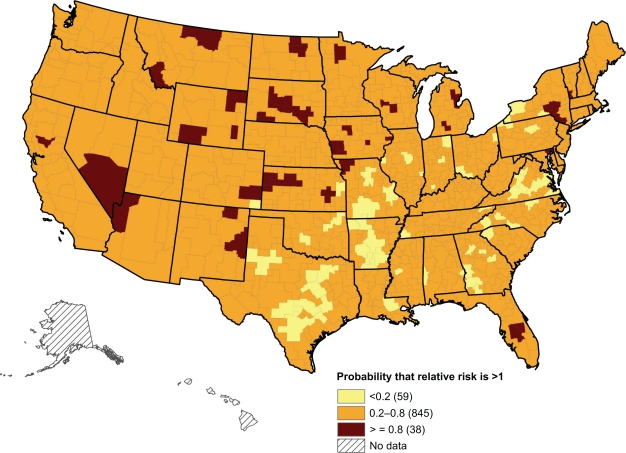
Methods: Almost 3.8 million COPD hospitalization records were extracted from Medicare claims for 1995-2006, and the total population of eligible Medicare beneficiaries was extracted from the Medicare enrollment records to calculate COPD hospitalization rates by Health Service Area (HSA), (n = 949). Spatial cluster analysis and Bayesian hierarchical spatial modeling were used to characterize the geography of COPD hospitalizations.
Results: The overall COPD hospitalization rate was 11.30 per 1,000 beneficiaries for the aggregated period 1995-2006. HSA-level COPD hospitalization rates had a median of 11.7 and a range of 3.0 (Cache, UT) to 76.3 (Pike, KY). Excessive hospitalization risk was concentrated in Appalachia, the southern Great Lakes, the Mississippi Delta, the Deep South, and west Texas. In the Bayesian spatial mixture model, 73% of variability of COPD hospitalization relative risk was attributed to unidentified regional social and physical environments shared by HSAs rather than to unique local HSA factors (27%).
Conclusion: We discovered distinct geographic patterns in COPD hospitalization rates and risks attributed to both regionally-shared environmental risk factors and HSA-unique environmental contexts. The correlates of these geographic patterns remain to be determined. Geographic comparisons of COPD hospitalization risk provide insights for better public health practice, policies, and programs for COPD prevention.
Keywords: COPD prevention; environmental risk factors; population; public health.
Figures

References
-
- Mannino DM. Chronic obstructive pulmonary disease: definition and epidemiology. Respir Care. 2003;48(12):1185–1191. 1191–1193. discussion. - PubMed
-
- Centers for Disease Control and Prevention Deaths from chronic obstructive pulmonary disease – United States, 2000–2005. MMWR. 2008;57(45) - PubMed
-
- Mannino D, Hom D, Akinbami L, Ford E, Redd S. Chronic obstructive pulmonary disease surveillance – United States, 1971–2000. WWMR. 2002;51(SS–6):1–16. - PubMed
-
- Menzin J, Boulanger L, Marton J, et al. The economic burden of chronic obstructive pulmonary disease (COPD) in a US Medicare population. Respir Med. 2008;102(9):1248–1256. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
