

Marital status and survival in pancreatic cancer patients: a SEER based analysis
- PMID: 21698253
- PMCID: PMC3115975
- DOI: 10.1371/journal.pone.0021052
Marital status and survival in pancreatic cancer patients: a SEER based analysis
Abstract
Background: Recent findings suggest that marital status affects survival in patients with different types of cancer. However, its role in the survival of patients with pancreatic ductal adenocarcinoma is unknown. In this study, we investigated whether there was an association between marital status and overall survival (OS) in patients with pancreatic ductal adenocarcinoma (PDAC).
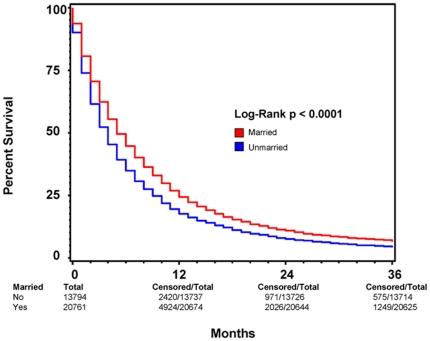
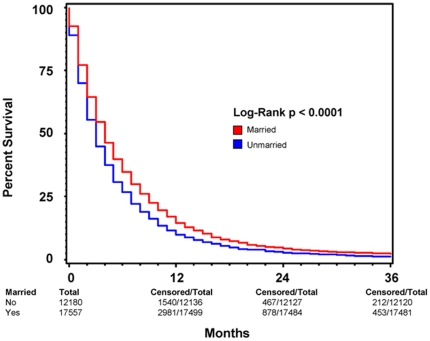
Methods: Adult patients diagnosed with PDAC between 1998 and 2003 with known marital statuses were identified from the Surveillance, Epidemiology, and End Results registry of the National Cancer Institute. OS for these patients was plotted using the Kaplan-Meier method. Comparative risks of mortality were evaluated by using univariate and multivariate-adjusted Cox regression models.
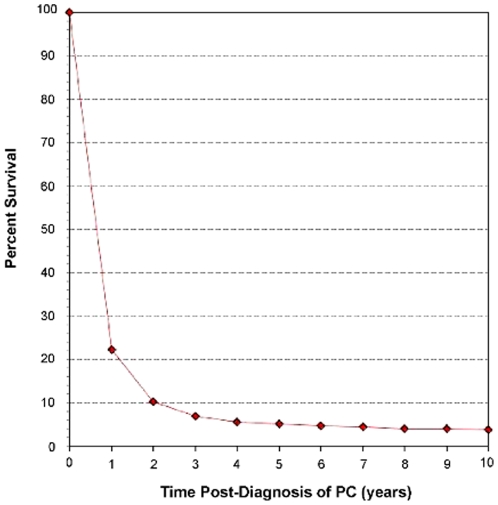
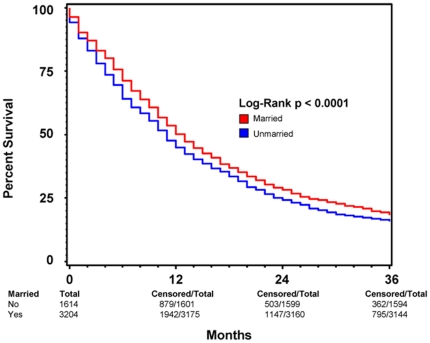
Results: Using Kaplan-Meier analysis, we found that the median overall survival of patients was 4 months and 3 months (p<0.001) for married and unmarried patients, respectively. Subgroup analysis on patients with cancer-directed surgery showed that the median survival was 16 months and 13 months (P<0.0005) for married and unmarried groups, respectively. Multivariate analysis adjusting for age, race, sex, stage, year of diagnosis, radiation therapy and cancer-directed surgery showed that patients who were married at the time of diagnosis had a significantly decreased risk of death at both 2 months (15% risk reduction) and 3 years (13% risk reduction) post diagnosis.
Conclusions: Marital status is an independent prognostic factor of both perioperative and long-term survival in patients with PDAC. This observation may suggest a suboptimally met psychosocial need among PDAC patients that is partially fulfilled by the support system provided by marriage.
Conflict of interest statement
Figures
References
-
- The American Cancer Society: Cancer Facts and Figures 2009. http://www.cancer.org/Research/CancerFactsFigures/index. Accessed February 23, 2010.
-
- National Cancer Institute: Surveillance Epidemiology and End Results Cancer Statistics Review 1975–2006. http://seer.cancer.gov/csr/1975_2006/index.html. Accessed February 23, 2010.
-
- Kaplan GA, Salonen JT, Cohen RD, Brand RJ, Syme SL, et al. Social connections and mortality from all causes and from cardiovascular disease: prospective evidence from eastern Finland. Am J Epidemiol. 1988;128:370–80. - PubMed
-
- Kravdal O. The impact of marital status on cancer survival. Soc Sci Med. 2001;52:357–68. - PubMed
-
- Kaplan EH, Meier P. Nonparametric estimation from incomplete observations. J Amer Statist Assn. 1958;53:457–481.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
