

Severe morbidity and mortality in untreated HIV-infected children in a paediatric care programme in Abidjan, Côte d'Ivoire, 2004-2009
- PMID: 21699728
- PMCID: PMC3138448
- DOI: 10.1186/1471-2334-11-182
Severe morbidity and mortality in untreated HIV-infected children in a paediatric care programme in Abidjan, Côte d'Ivoire, 2004-2009
Abstract
Background: Clinical evolution of HIV-infected children who have not yet initiated antiretroviral treatment (ART) is poorly understood in Africa. We describe severe morbidity and mortality of untreated HIV-infected children.
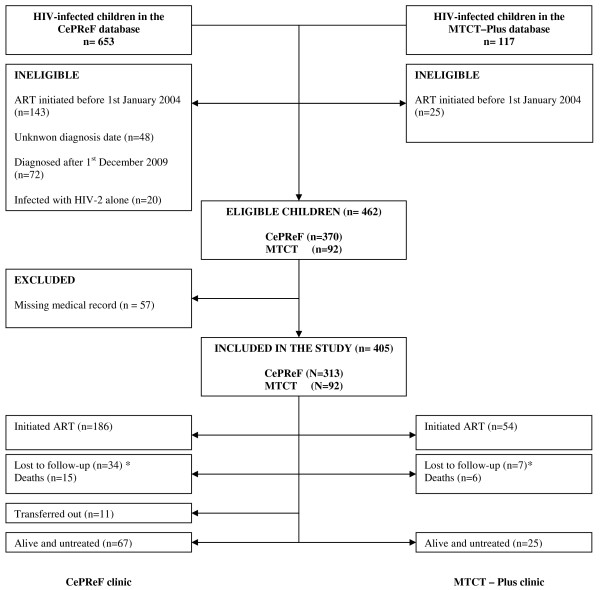
Methods: All HIV-infected children enrolled from 2004-2009 in a prospective HIV programme in two health facilities in Abidjan, Côte d'Ivoire, were eligible from their time of inclusion. Risks of severe morbidity (the first clinical event leading to death or hospitalisation) and mortality were documented retrospectively and estimated using cumulative incidence functions. Associations with baseline characteristics were assessed by competing risk regression models between outcomes and antiretroviral initiation.
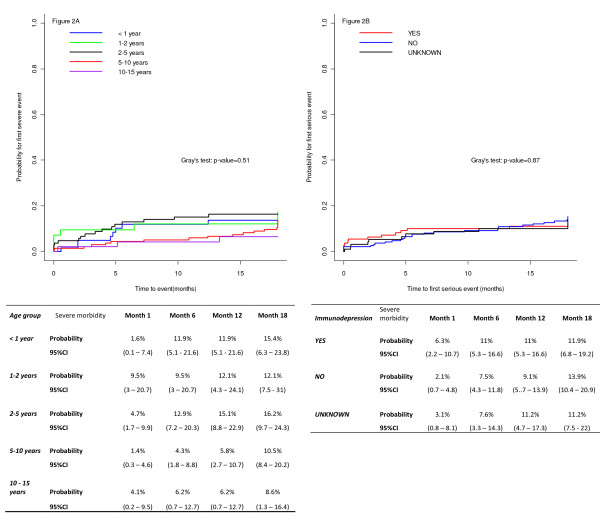
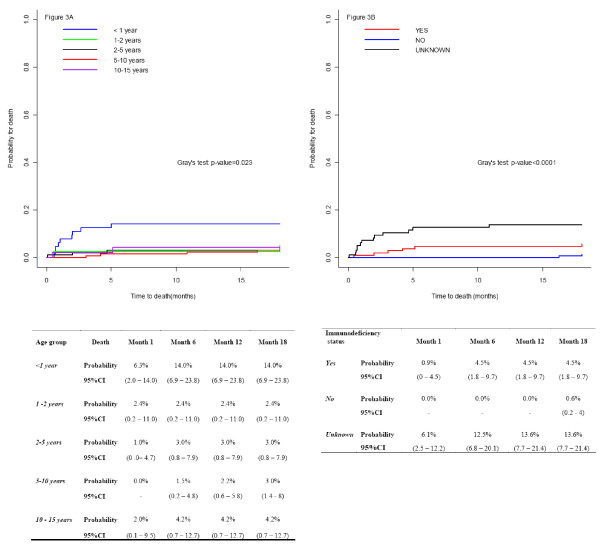
Results: 405 children were included at a median age of 4.5 years; at baseline, 66.9% were receiving cotrimoxazole prophylaxis, and 27.7% met the 2006 WHO criteria for immunodeficiency by age. The risk of developing a severe morbid event was 14% (95%CI: 10.7 - 17.8) at 18 months; this risk was lower in children previously exposed to any prevention of mother-to-child-transmission (PMTCT) intervention (adjusted subdistribution hazard ratio [sHR]: 0.16, 95% CI: 0.04 - 0.71) versus those without known exposure. Cumulative mortality reached 5.5% (95%CI: 3.5 - 8.1) at 18 months. Mortality was associated with immunodeficiency (sHR: 6.02, 95% CI: 1.28-28.42).
Conclusions: Having benefited from early access to care minimizes the severe morbidity risk for children who acquire HIV. Despite the receipt of cotrimoxazole prophylaxis, the risk of severe morbidity and mortality remains high in untreated HIV-infected children. Such evidence adds arguments to promote earlier access to ART in HIV-infected children in Africa and improve care interventions in a context where treatment is still not available to all.
Figures
References
-
- World Health Organization.UNAIDS. 2009 Report on global AIDS epidemic. Geneva, UNAIDS; 2009.
-
- Anaky M, Duvignac J, Wemin L, Kouakoussui A, Karcher S, Touré S, Seyler C, Fassinou P, Dabis F, N'Dri-Yoman T, Anglaret X, Leroy V. Scaling up antiretroviral therapy for HIV-infected children in Côte d'Ivoire: determinants of survival and loss to programme. Bull World Health Organ. 2010;88(7):490–499. doi: 10.2471/BLT.09.068015. - DOI - PMC - PubMed
-
- Stringer EM, Ekouevi DK, Coetzee D, Tih PM, Creek TL, Stinson K, Giganti MJ, Welty TK, Chintu N, Chi BH, Wilfert CM, Shaffer N, Dabis F, Stringer JS. PEARL Study Team. Coverage of nevirapine-based services to prevent mother-to-child HIV transmission in 4 African countries. JAMA. 2010;304(3):293–302. doi: 10.1001/jama.2010.990. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
