

Peripheral vascular decoupling in porcine endotoxic shock
- PMID: 21700890
- PMCID: PMC3174791
- DOI: 10.1152/japplphysiol.00066.2011
Peripheral vascular decoupling in porcine endotoxic shock
Abstract
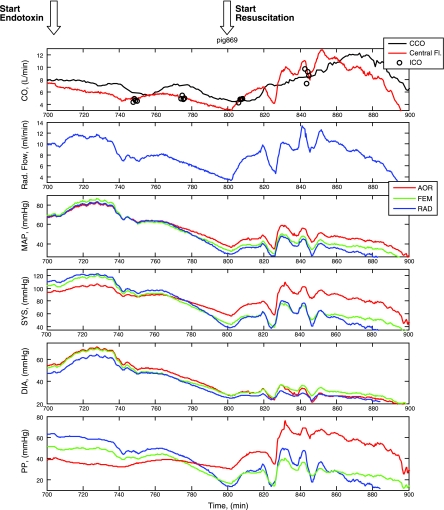
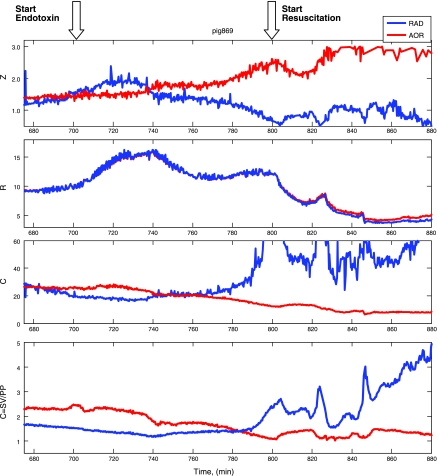
Cardiac output measurement from arterial pressure waveforms presumes a defined relationship between the arterial pulse pressure (PP), vascular compliance (C), and resistance (R). Cardiac output estimates degrade if these assumptions are incorrect. We hypothesized that sepsis would differentially alter central and peripheral vasomotor tone, decoupling the usual pressure wave propagation from central to peripheral sites. We assessed arterial input impedance (Z), C, and R from central and peripheral arterial pressures, and aortic blood flow in an anesthetized porcine model (n = 19) of fluid resuscitated endotoxic shock induced by endotoxin infusion (7 μg·kg⁻¹·h⁻¹ increased to 14 and 20 μg·kg⁻¹·h⁻¹ every 10 min and stopped when mean arterial pressure <40 mmHg or Sv(O₂) < 45%). Aortic, femoral, and radial artery pressures and aortic and radial artery flows were measured. Z was calculated by FFT of flow and pressure data. R and C were derived using a two-element Windkessel model. Arterial PP increased from aortic to femoral and radial sites. During stable endotoxemia with fluid resuscitation, aortic and radial blood flows returned to or exceeded baseline while mean arterial pressure remained similarly decreased at all three sites. However, aortic PP exceeded both femoral and radial arterial PP. Although Z, R, and C derived from aortic and radial pressure and aortic flow were similar during baseline, Z increases and C decreases when derived from aortic pressure whereas Z decreases and C increases when derived from radial pressure, while R decreased similarly with both pressure signals. This central-to-peripheral vascular tone decoupling, as quantified by the difference in calculated Z and C from aortic and radial artery pressure, may explain the decreasing precision of peripheral arterial pressure profile algorithms in assessing cardiac output in septic shock patients and suggests that different algorithms taking this vascular decoupling into account may be necessary to improve their precision in this patient population.
Figures

References
-
- Bernard GR, Reines HD, Halushka PV, Higgins SB, Metz CA, Swindell BB, Wright PE, Watts FL, Vrbanac JJ. Prostacyclin and thromboxane-A2 formation is increased in human sepsis syndrome—Effects of cyclooxygenase inhibition. Am Rev Respir Dis 144: 1095–1101, 1991 - PubMed
-
- Calandra T, Gerain J, Heumann D, Baumgartner JD, Glauser MP. High circulating levels of interleukin-6 in patients with septic shock: Evolution during sepsis, prognostic value, and interplay with other cytokines. Am J Med 91: 23–29, 1991 - PubMed
-
- Chaney JC, Derdak S. Minimally invasive hemodynamic monitoring for the intensivist: current and emerging technology. Crit Care Med 30: 2338–2345, 2002 - PubMed
-
- Cholley BP, Shroff SG, Sandelski J, Korcarz C, Balasia BA, Jain S, Berger DS, Murphy MB, Marcus RH, Lang RM. Differential effects of chronic oral antihypertensive therapies on systemic arterial circulation and ventricular energetics in African-American patients. Circulation 91: 1052–1062, 1995 - PubMed
-
- Della Rocca G, Cecconi M, Costa MG. Mini invasive hemodynamic monitoring: from arterial pressure to cardiac output. SIGNA VITAE 3: S7–S9, 2008
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous