

Armed and targeted measles virus for chemovirotherapy of pancreatic cancer
- PMID: 21701532
- PMCID: PMC3914720
- DOI: 10.1038/cgt.2011.30
Armed and targeted measles virus for chemovirotherapy of pancreatic cancer
Abstract
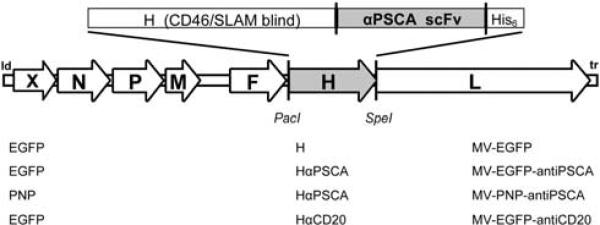
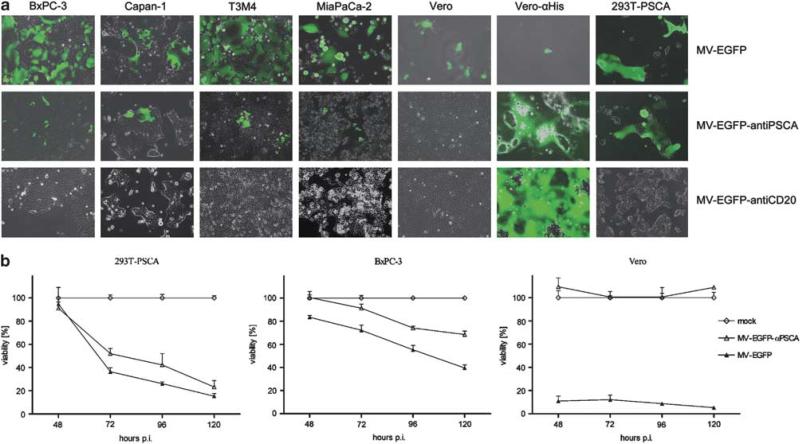
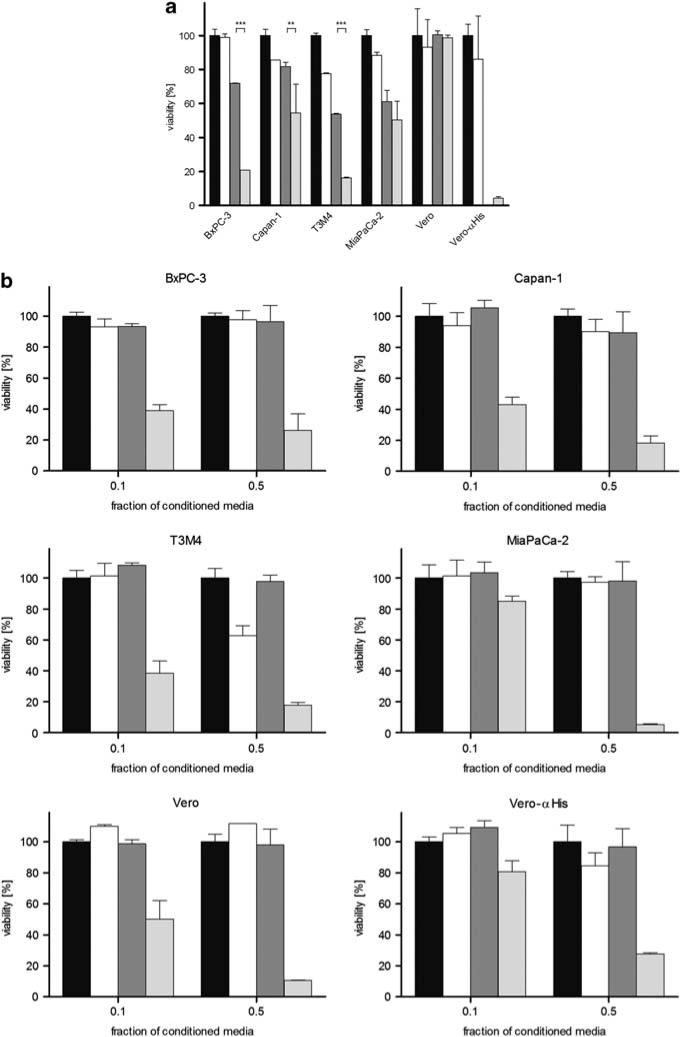
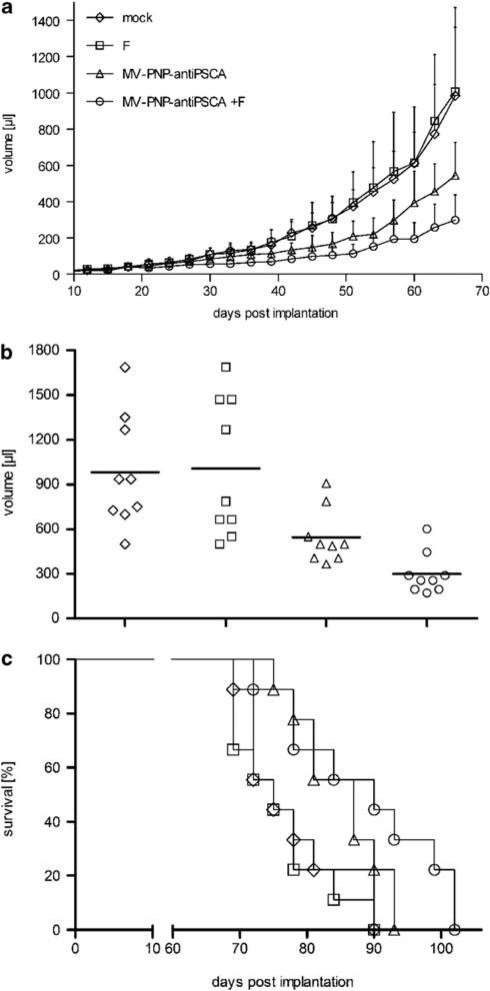
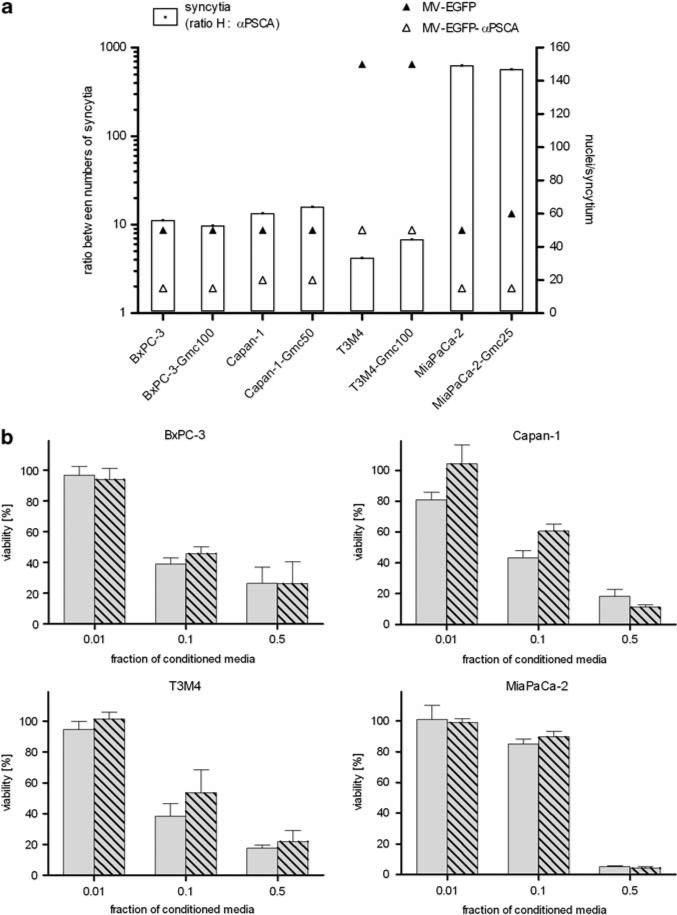
No curative therapy is currently available for locally advanced or metastatic pancreatic cancer. Therefore, new therapeutic approaches must be considered. Measles virus (MV) vaccine strains have shown promising oncolytic activity against a variety of tumor entities. For specific therapy of pancreatic cancer, we generated a fully retargeted MV that enters cells exclusively through the prostate stem cell antigen (PSCA). Besides a high-membrane frequency on prostate cancer cells, this antigen is expressed on pancreatic adenocarcinoma, but not on non-neoplastic tissue. PSCA expression levels differ within heterogeneous tumor bulks and between human pancreatic cell lines, and we could show specific infection of pancreatic adenocarcinoma cell lines with both high- and low-level PSCA expression. Furthermore, we generated a fully retargeted and armed MV-PNP-anti-PSCA to express the prodrug convertase purine nucleoside phosphorylase (PNP). PNP, which activates the prodrug fludarabine effectively, enhanced the oncolytic efficacy of the virus on infected and bystander cells. Beneficial therapeutic effects were shown in a pancreatic cancer xenograft model. Moreover, in the treatment of gemcitabine-resistant pancreatic adenocarcinoma cells, no cross-resistance to both MV oncolysis and activated prodrug was detected.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Hidalgo M. Pancreatic cancer. N Engl J Med. 2010;362:1605–1617. - PubMed
-
- Alberts SR, Gores GJ, Kim GP, Roberts LR, Kendrick ML, Rosen CB, et al. Treatment options for hepatobiliary and pancreatic cancer. Mayo Clin Proc. 2007;82:628–637. - PubMed
-
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25:1960–1966. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
