

Sequential FDG-PET and induction chemotherapy in locally advanced adenocarcinoma of the Oesophago-gastric junction (AEG): the Heidelberg Imaging program in Cancer of the oesophago-gastric junction during Neoadjuvant treatment: HICON trial
- PMID: 21702914
- PMCID: PMC3149600
- DOI: 10.1186/1471-2407-11-266
Sequential FDG-PET and induction chemotherapy in locally advanced adenocarcinoma of the Oesophago-gastric junction (AEG): the Heidelberg Imaging program in Cancer of the oesophago-gastric junction during Neoadjuvant treatment: HICON trial
Abstract
Background: 18-Fluorodeoxyglucose-PET (18F-FDG-PET) can be used for early response assessment in patients with locally advanced adenocarcinomas of the oesophagogastric junction (AEG) undergoing neoadjuvant chemotherapy. It has been recently shown in the MUNICON trials that response-guided treatment algorithms based on early changes of the FDG tumor uptake detected by PET are feasible and that they can be implemented into clinical practice. Only 40%-50% of the patients respond metabolically to therapy. As metabolic non-response is known to be associated with a dismal prognosis, metabolic non-responders are increasingly treated with alternative neoadjuvant chemotherapies or chemoradiation in order to improve their clinical outcome. We plan to investigate whether PET can be used as response assessment during radiochemotherapy given as salvage treatment in early metabolic non-responders to standard chemotherapy.
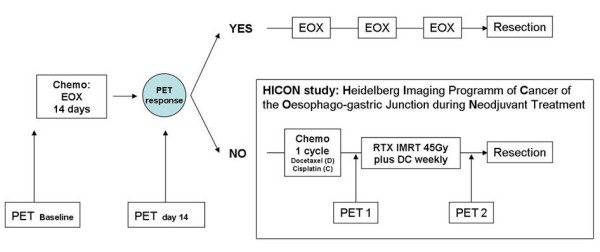
Methods/design: The HICON trial is a prospective, non-randomized, explorative imaging study evaluating the value of PET as a predictor of histopathological response in metabolic non-responders. Patients with resectable AEG type I and II according to Siewerts classification, staged cT3/4 and/or cN+ and cM0 by endoscopic ultrasound, spiral CT or MRI and FDG-PET are eligible. Tumors must be potentially R0 resectable and must have a sufficient FDG-baseline uptake. Only metabolic non-responders, showing a < 35% decrease of SUV two weeks after the start of neoadjuvant chemotherapy are eligible for the study and are taken to intensified taxane-based RCT (chemoradiotherapy (45 Gy) before surgery. 18FDG-PET scans will be performed before ( = Baseline) and after 14 days of standard neoadjuvant therapy as well as after the first cycle of salvage docetaxel/cisplatin chemotherapy (PET 1) and at the end of radiochemotherapy (PET2). Tracer uptake will be assessed semiquantitatively using standardized uptake values (SUV). The percentage difference ΔSUV = 100 (SUV Baseline - SUV PET1)/SUV Baseline will be calculated and assessed as an early predictor of histopathological response. In a secondary analysis, the association between the difference SUV PET1 - SUV PET2 and histopathological response will be evaluated.
Discussion: The aim of this study is to investigate the potential of sequential 18FDG-PET in predicting histopathological response in AEG tumors to salvage neoadjuvant radiochemotherapy in patients who do not show metabolic response to standard neoadjuvant chemotherapy.
Trial registration: ClinicalTrials.gov NCT01271322.
Similar articles
-
Locally advanced esophageal adenocarcinoma: response to neoadjuvant chemotherapy and survival predicted by ([18F])FDG-PET/CT.Acta Oncol. 2012 May;51(5):636-44. doi: 10.3109/0284186X.2011.643822. Epub 2012 Jan 2. Acta Oncol. 2012. PMID: 22208782
-
Assessment of diffusion-weighted MRI and 18F-fluoro-deoxyglucose PET/CT in monitoring early response to neoadjuvant chemotherapy in adenocarcinoma of the esophagogastric junction.J Gastrointestin Liver Dis. 2013 Mar;22(1):45-52. J Gastrointestin Liver Dis. 2013. PMID: 23539390
-
PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: the MUNICON phase II trial.Lancet Oncol. 2007 Sep;8(9):797-805. doi: 10.1016/S1470-2045(07)70244-9. Lancet Oncol. 2007. PMID: 17693134 Clinical Trial.
-
Optimizing neoadjuvant chemotherapy through the use of early response evaluation by positron emission tomography.Recent Results Cancer Res. 2012;196:201-11. doi: 10.1007/978-3-642-31629-6_14. Recent Results Cancer Res. 2012. PMID: 23129376 Review.
-
Prognostic significance of SUV on PET/CT in patients with localised oesophagogastric junction cancer receiving neoadjuvant chemotherapy/chemoradiation:a systematic review and meta-analysis.Br J Radiol. 2012 Sep;85(1017):e694-701. doi: 10.1259/bjr/29946900. Epub 2012 Feb 14. Br J Radiol. 2012. PMID: 22337686 Free PMC article.
Cited by
-
Contrast-enhanced ultrasonography assessment of gastric cancer response to neoadjuvant chemotherapy.World J Gastroenterol. 2012 Dec 21;18(47):7026-32. doi: 10.3748/wjg.v18.i47.7026. World J Gastroenterol. 2012. PMID: 23323004 Free PMC article.
-
A phase II study for metabolic in vivo response monitoring with sequential 18FDG-PET-CT during treatment with the EGFR-monoclonal-antibody cetuximab in metastatic colorectal cancer: the Heidelberg REMOTUX trial.BMC Cancer. 2012 Mar 22;12:108. doi: 10.1186/1471-2407-12-108. BMC Cancer. 2012. PMID: 22439666 Free PMC article. Clinical Trial.
-
Perioperative therapy for locally advanced gastroesophageal cancer: current controversies and consensus of care.J Hematol Oncol. 2013 Sep 5;6:66. doi: 10.1186/1756-8722-6-66. J Hematol Oncol. 2013. PMID: 24010946 Free PMC article. Review.
-
The role of ¹⁸F-FDG PET imaging in upper gastrointestinal malignancies.Curr Treat Options Oncol. 2014 Sep;15(3):351-64. doi: 10.1007/s11864-014-0301-9. Curr Treat Options Oncol. 2014. PMID: 25064175 Review.
-
Current strategies in chemoradiation for esophageal cancer.J Gastrointest Oncol. 2014 Jun;5(3):156-65. doi: 10.3978/j.issn.2078-6891.2014.033. J Gastrointest Oncol. 2014. PMID: 24982764 Free PMC article. Review.
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
