

Phosphodiesterase-4 inhibition combined with isoniazid treatment of rabbits with pulmonary tuberculosis reduces macrophage activation and lung pathology
- PMID: 21703411
- PMCID: PMC3123788
- DOI: 10.1016/j.ajpath.2011.03.039
Phosphodiesterase-4 inhibition combined with isoniazid treatment of rabbits with pulmonary tuberculosis reduces macrophage activation and lung pathology
Abstract
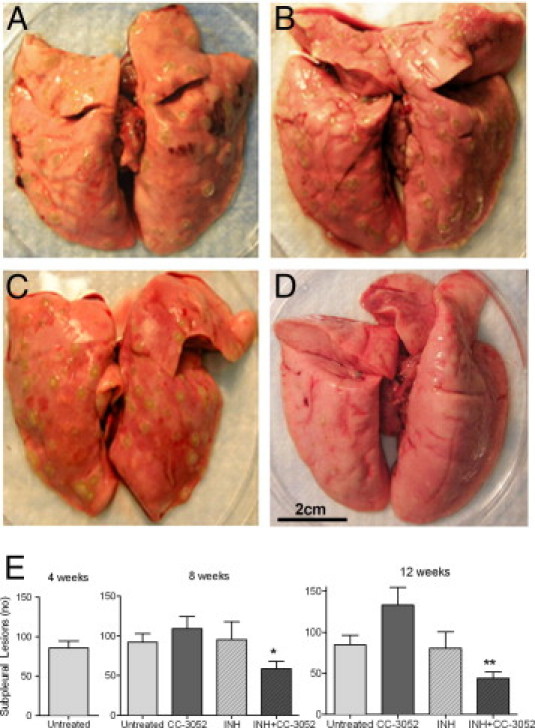
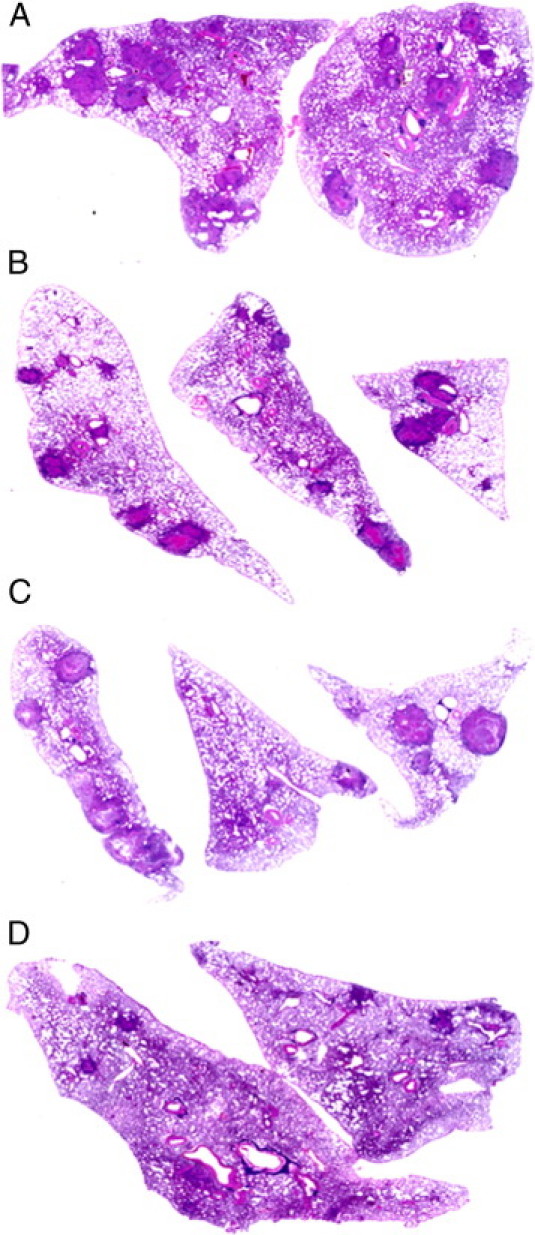
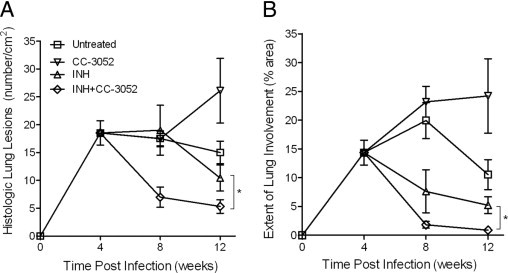
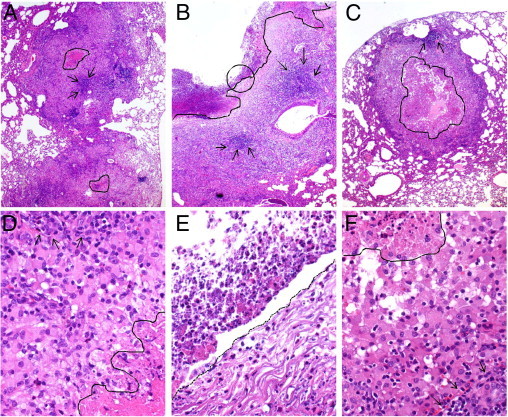
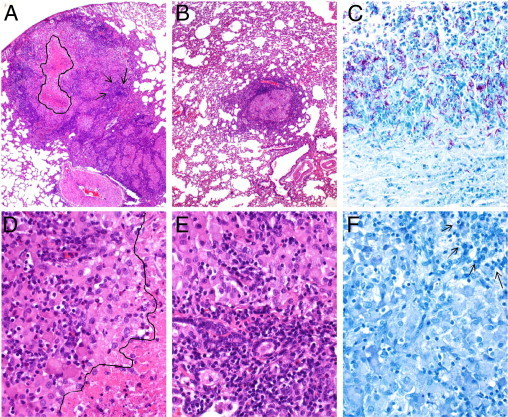
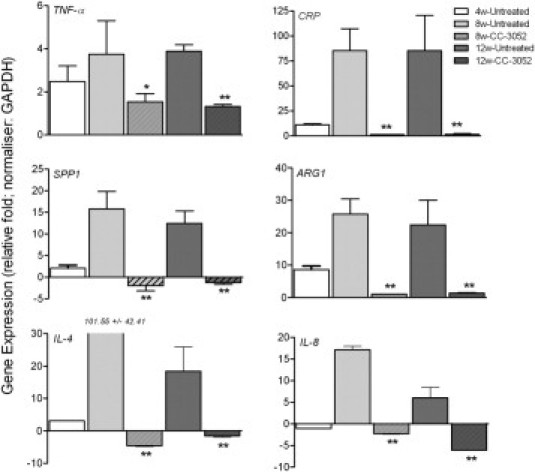
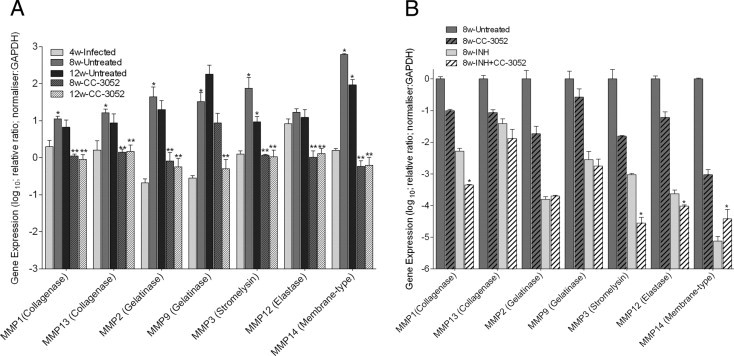
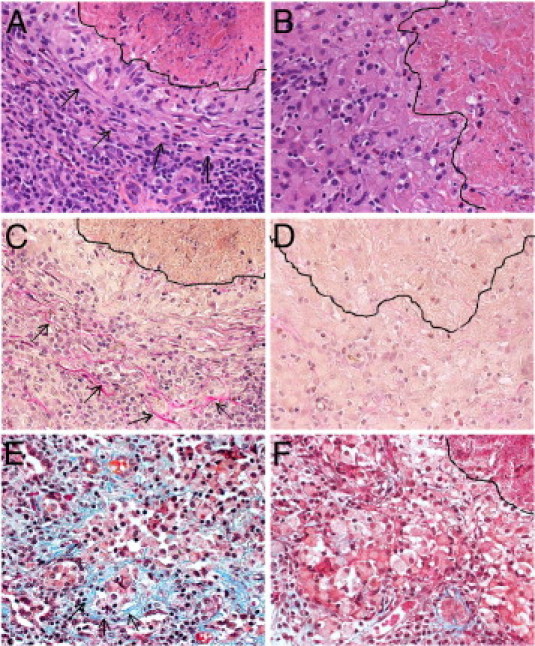
Tuberculosis (TB) is responsible for significant morbidity and mortality worldwide. Even after successful microbiological cure of TB, many patients are left with residual pulmonary damage that can lead to chronic respiratory impairment and greater risk of additional TB episodes due to reinfection with Mycobacterium tuberculosis. Elevated levels of the proinflammatory cytokine tumor necrosis factor-α and several other markers of inflammation, together with expression of matrix metalloproteinases, have been associated with increased risk of pulmonary fibrosis, tissue damage, and poor treatment outcomes in TB patients. In this study, we used a rabbit model of pulmonary TB to evaluate the impact of adjunctive immune modulation, using a phosphodiesterase-4 inhibitor that dampens the innate immune response, on the outcome of treatment with the antibiotic isoniazid. Our data show that cotreatment of M. tuberculosis infected rabbits with the phosphodiesterase-4 inhibitor CC-3052 plus isoniazid significantly reduced the extent of immune pathogenesis, compared with antibiotic alone, as determined by histologic analysis of infected tissues and the expression of genes involved in inflammation, fibrosis, and wound healing in the lungs. Combined treatment with an antibiotic and CC-3052 not only lessened disease but also improved bacterial clearance from the lungs. These findings support the potential for adjunctive immune modulation to improve the treatment of pulmonary TB and reduce the risk of chronic respiratory impairment.
Copyright © 2011 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Phosphodiesterase-4 inhibition alters gene expression and improves isoniazid-mediated clearance of Mycobacterium tuberculosis in rabbit lungs.PLoS Pathog. 2011 Sep;7(9):e1002262. doi: 10.1371/journal.ppat.1002262. Epub 2011 Sep 15. PLoS Pathog. 2011. PMID: 21949656 Free PMC article.
-
Adjunctive Phosphodiesterase-4 Inhibitor Therapy Improves Antibiotic Response to Pulmonary Tuberculosis in a Rabbit Model.EBioMedicine. 2016 Jan 14;4:104-14. doi: 10.1016/j.ebiom.2016.01.015. eCollection 2016 Feb. EBioMedicine. 2016. PMID: 26981575 Free PMC article.
-
Phosphodiesterase 4 inhibition reduces innate immunity and improves isoniazid clearance of Mycobacterium tuberculosis in the lungs of infected mice.PLoS One. 2011 Feb 25;6(2):e17091. doi: 10.1371/journal.pone.0017091. PLoS One. 2011. PMID: 21364878 Free PMC article.
-
Thalidomide and Phosphodiesterase 4 Inhibitors as Host Directed Therapeutics for Tuberculous Meningitis: Insights From the Rabbit Model.Front Cell Infect Microbiol. 2020 Jan 14;9:450. doi: 10.3389/fcimb.2019.00450. eCollection 2019. Front Cell Infect Microbiol. 2020. PMID: 32010638 Free PMC article. Review.
-
Breaking the Cycle: Matrix Metalloproteinase Inhibitors as an Alternative Approach in Managing Tuberculosis Pathogenesis and Progression.ACS Infect Dis. 2024 Aug 9;10(8):2567-2583. doi: 10.1021/acsinfecdis.4c00385. Epub 2024 Jul 22. ACS Infect Dis. 2024. PMID: 39038212 Review.
Cited by
-
The Interplay Between Systemic Inflammation, Oxidative Stress, and Tissue Remodeling in Tuberculosis.Antioxid Redox Signal. 2021 Feb 20;34(6):471-485. doi: 10.1089/ars.2020.8124. Epub 2020 Jun 19. Antioxid Redox Signal. 2021. PMID: 32559410 Free PMC article. Review.
-
Cytokine Biosignature of Active and Latent Mycobacterium Tuberculosis Infection in Children.Pathogens. 2021 Apr 24;10(5):517. doi: 10.3390/pathogens10050517. Pathogens. 2021. PMID: 33923293 Free PMC article.
-
Combined chemical genetics and data-driven bioinformatics approach identifies receptor tyrosine kinase inhibitors as host-directed antimicrobials.Nat Commun. 2018 Jan 24;9(1):358. doi: 10.1038/s41467-017-02777-6. Nat Commun. 2018. PMID: 29367740 Free PMC article.
-
Adjunctive TNF inhibition with standard treatment enhances bacterial clearance in a murine model of necrotic TB granulomas.PLoS One. 2012;7(6):e39680. doi: 10.1371/journal.pone.0039680. Epub 2012 Jun 27. PLoS One. 2012. PMID: 22761866 Free PMC article.
-
Phosphodiesterase inhibitors as adjunctive therapies for tuberculosis.EBioMedicine. 2016 Feb 9;4:7-8. doi: 10.1016/j.ebiom.2016.02.016. eCollection 2016 Feb. EBioMedicine. 2016. PMID: 26981560 Free PMC article. No abstract available.
References
-
- Treatment of tuberculosis. MMWR Morb Mortal Wkly Rep. 2003;52:1–77.
-
- de Valliere S., Barker R.D. Residual lung damage after completion of treatment for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2004;8:767–771. - PubMed
-
- Pasipanodya J.G., Miller T.L., Vecino M., Munguia G., Garmon R., Bae S., Drewyer G., Weis S.E. Pulmonary impairment after tuberculosis. Chest. 2007;131:1817–1824. - PubMed
-
- Park J.H., Na J.O., Kim E.K., Lim C.M., Shim T.S., Lee S.D., Kim W.S., Kim D.S., Kim W.D., Koh Y. The prognosis of respiratory failure in patients with tuberculous destroyed lung. Int J Tuberc Lung Dis. 2001;5:963–967. - PubMed
-
- Ross J., Ehrlich R.I., Hnizdo E., White N., Churchyard G.J. Excess lung function decline in gold miners following pulmonary tuberculosis. Thorax. 2010;65:963–967. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
