

The impact of extra cardiac comorbidities on pressure volume relations in heart failure and preserved ejection fraction
- PMID: 21703526
- PMCID: PMC3124657
- DOI: 10.1016/j.cardfail.2011.03.010
The impact of extra cardiac comorbidities on pressure volume relations in heart failure and preserved ejection fraction
Abstract
Background: Extracardiac comorbidities are common in patients with heart failure and a preserved ejection fraction (HFPEF). We sought to evaluate the relationship between comorbidities and ventricular structure and function in patients with HFPEF through evaluation of pressure-volume analysis.
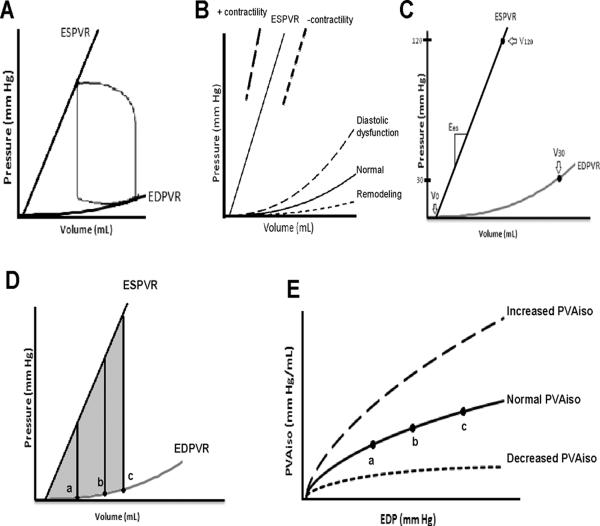
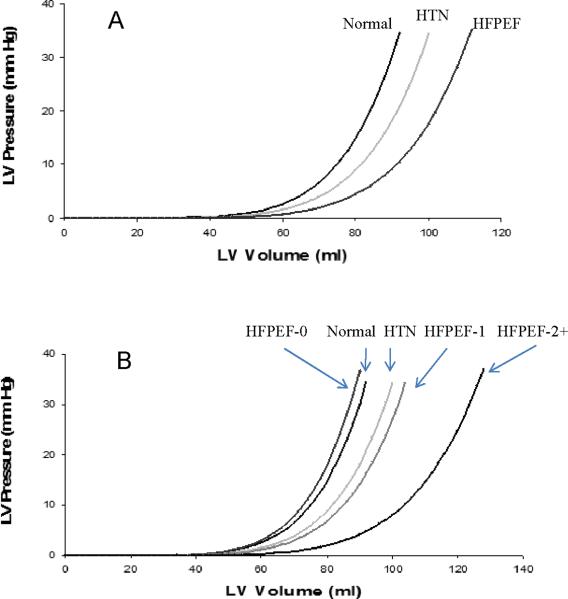
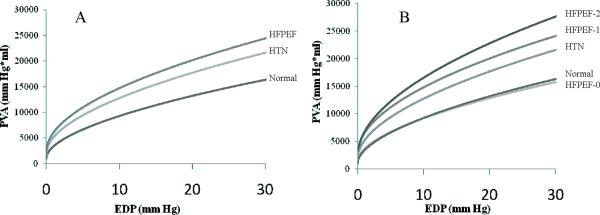
Methods and results: Two hundred twenty Chinese patients with a preserved ejection fraction who were either healthy (n = 75), hypertensive without heart failure (HTN; n = 89), or hypertensive with HFPEF (HFPEF; n = 56) were studied. Using echocardiographic measures, estimated end-systolic and end-diastolic pressure-volume relationships, and the area between them as a function of EDP, the isovolumic pressure-volume areas (PVA(iso)), were calculated. Ventricular capacitance, as measured by V(30), was larger in patients with HFPEF compared with normal control subjects and tended to be larger compared with hypertensive control subjects. The presence of diabetes and renal insufficiency was independently associated with greater ventricular capacitance in patients with HFPEF. The PVA(iso) was increased in patients with HFPEF compared with HTN and normal control subjects, and in particular, it was increased in HFPEF patients with multiple comorbidities.
Conclusions: The presence of comorbid conditions is associated with altered pressure-volume relations and enhanced pump function in subjects with HFPEF, supporting an important role for extracardiac comorbidities in the pathophysiology of patients with this condition.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Impaired systolic function by strain imaging in heart failure with preserved ejection fraction.J Am Coll Cardiol. 2014 Feb 11;63(5):447-56. doi: 10.1016/j.jacc.2013.09.052. Epub 2013 Oct 30. J Am Coll Cardiol. 2014. PMID: 24184245 Free PMC article. Clinical Trial.
-
Comorbidity and ventricular and vascular structure and function in heart failure with preserved ejection fraction: a community-based study.Circ Heart Fail. 2012 Nov;5(6):710-9. doi: 10.1161/CIRCHEARTFAILURE.112.968594. Epub 2012 Oct 17. Circ Heart Fail. 2012. PMID: 23076838 Free PMC article.
-
Cardiovascular features of heart failure with preserved ejection fraction versus nonfailing hypertensive left ventricular hypertrophy in the urban Baltimore community: the role of atrial remodeling/dysfunction.J Am Coll Cardiol. 2007 Jan 16;49(2):198-207. doi: 10.1016/j.jacc.2006.08.050. Epub 2006 Dec 29. J Am Coll Cardiol. 2007. PMID: 17222731
-
Sudden death in heart failure with preserved ejection fraction and beyond: an elusive target.Heart Fail Rev. 2019 Nov;24(6):847-866. doi: 10.1007/s10741-019-09804-2. Heart Fail Rev. 2019. PMID: 31147814 Review.
-
Advance in the pharmacological and comorbidities management of heart failure with preserved ejection fraction: evidence from clinical trials.Heart Fail Rev. 2024 Mar;29(2):305-320. doi: 10.1007/s10741-023-10338-x. Epub 2023 Aug 10. Heart Fail Rev. 2024. PMID: 37561223 Review.
Cited by
-
Age, Gender and Load-Related Influences on Left Ventricular Geometric Remodeling, Systolic Mid-Wall Function, and NT-ProBNP in Asymptomatic Asian Population.PLoS One. 2016 Jun 9;11(6):e0156467. doi: 10.1371/journal.pone.0156467. eCollection 2016. PLoS One. 2016. PMID: 27280886 Free PMC article.
-
A multidimensional sight on cardiac failure: uncovered from structural to molecular level.Heart Fail Rev. 2017 May;22(3):357-370. doi: 10.1007/s10741-017-9610-y. Heart Fail Rev. 2017. PMID: 28474325 Review.
-
Theoretical considerations for a left atrial pump in heart failure with preserved ejection fraction.Heart Fail Rev. 2023 Mar;28(2):273-280. doi: 10.1007/s10741-021-10121-w. Epub 2021 May 12. Heart Fail Rev. 2023. PMID: 33977494 Review.
-
Current treatment of heart failure with preserved ejection fraction: should we add life to the remaining years or add years to the remaining life?Cardiol Res Pract. 2013;2013:130724. doi: 10.1155/2013/130724. Epub 2013 Oct 24. Cardiol Res Pract. 2013. PMID: 24251065 Free PMC article. Review.
-
Mimicking the cardiac cycle in intact cardiomyocytes using diastolic and systolic force clamps; measuring power output.Cardiovasc Res. 2016 Jul 1;111(1):66-73. doi: 10.1093/cvr/cvw072. Epub 2016 Apr 1. Cardiovasc Res. 2016. PMID: 27037258 Free PMC article.
References
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–9. - PubMed
-
- Fonarow GC, Stough WG, Abraham WT, Albert NM, Gheorghiade M, Greenberg BH, et al. Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF Registry. J Am Coll Cardiol. 2007;50:768–77. - PubMed
-
- Klapholz M, Maurer M, Lowe AM, Messineo F, Meisner JS, Mitchell J, et al. Hospitalization for heart failure in the presence of a preserved left ventricular ejection fraction: results of the New York Heart Failure Registry. J Am Coll Cardiol. 2004;43:1432–8. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–9. - PubMed
-
- Tribouilloy C, Rusinaru D, Mahjoub H, Souliere V, Levy F, Peltier M, et al. Prognosis of heart failure with preserved ejection fraction: a 5 year prospective population-based study. Eur Heart J. 2008;29:339–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
