

Vitamin D supplementation during pregnancy: double-blind, randomized clinical trial of safety and effectiveness
- PMID: 21706518
- PMCID: PMC3183324
- DOI: 10.1002/jbmr.463
Vitamin D supplementation during pregnancy: double-blind, randomized clinical trial of safety and effectiveness
Erratum in
- J Bone Miner Res. 2011 Dec; 26(12):3001
Abstract
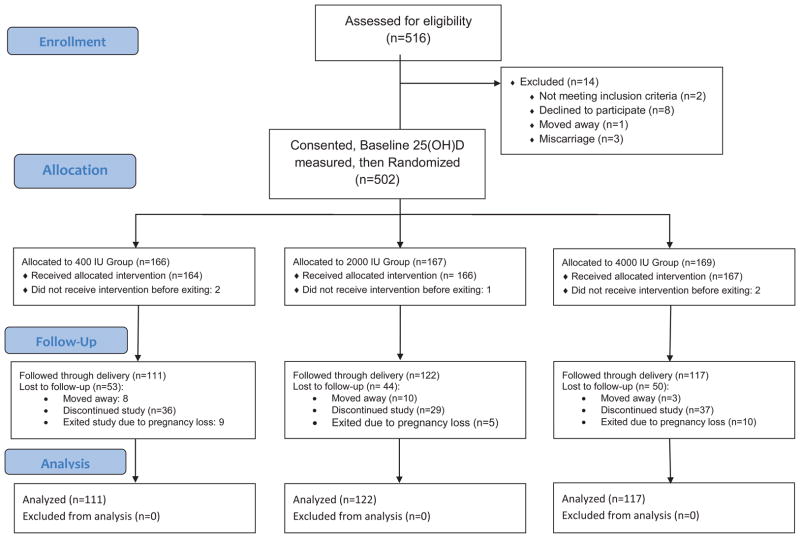
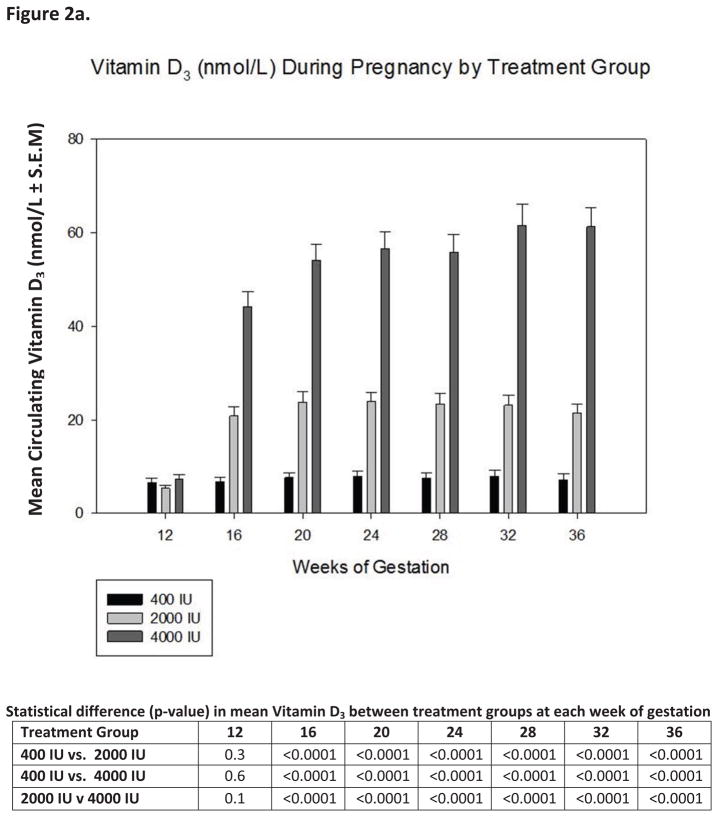
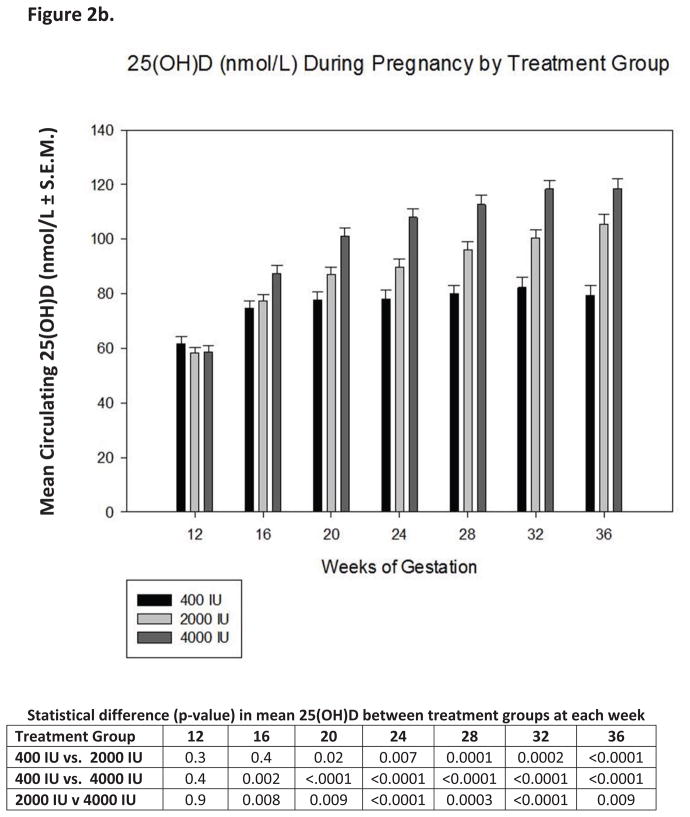
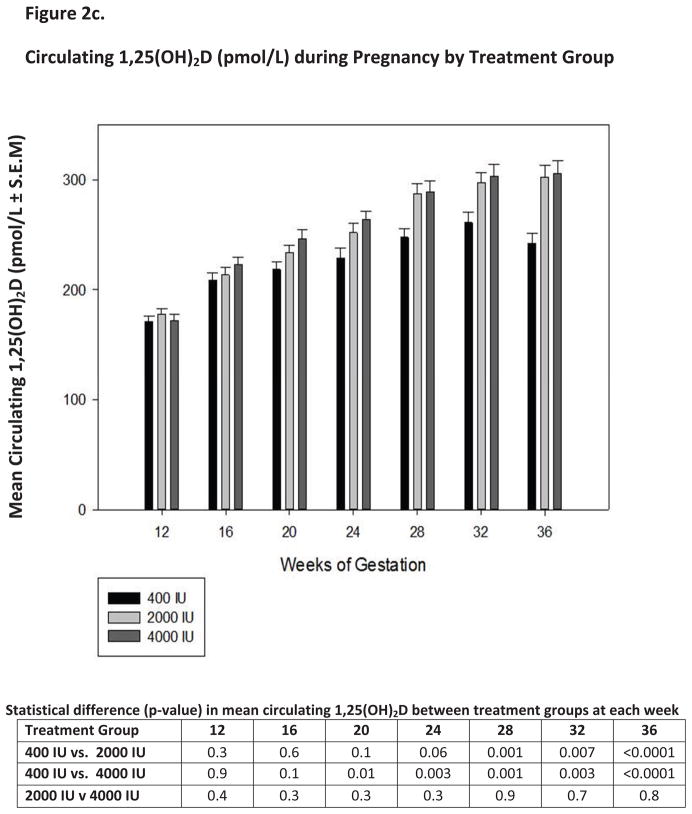
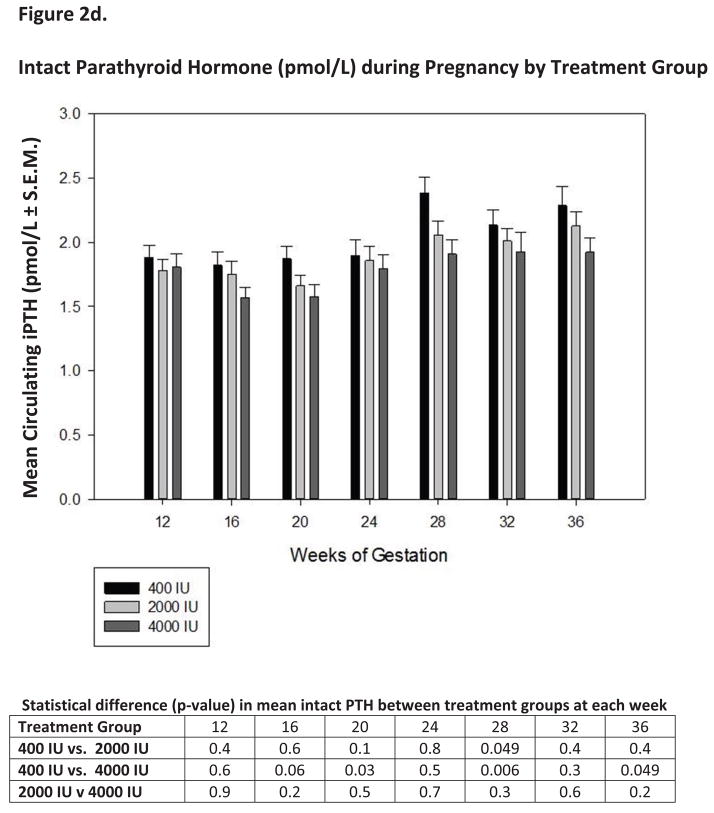
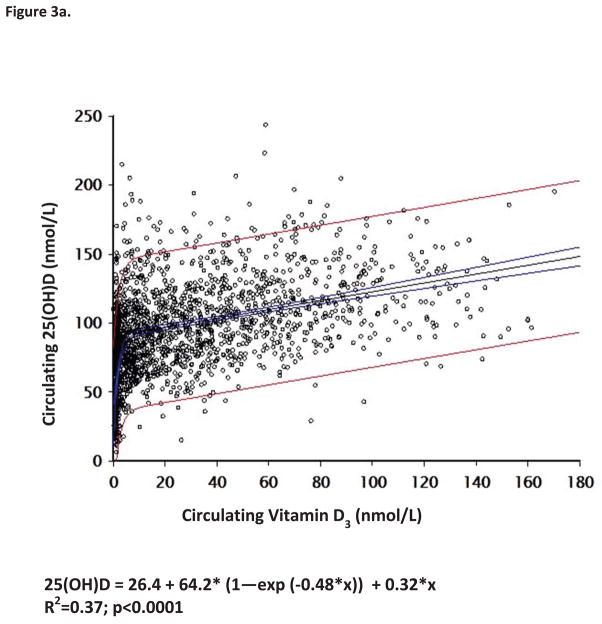
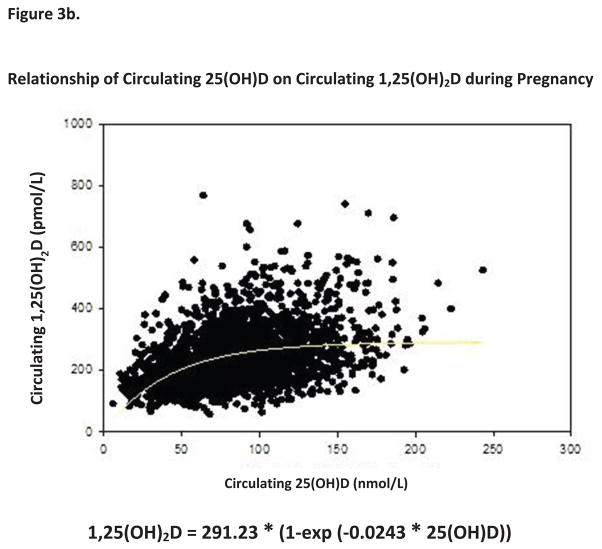
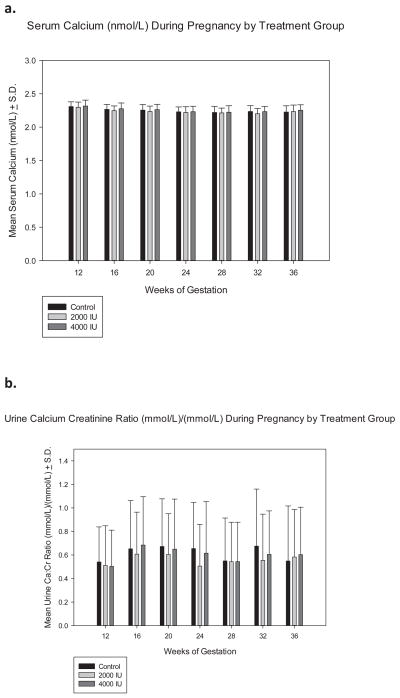
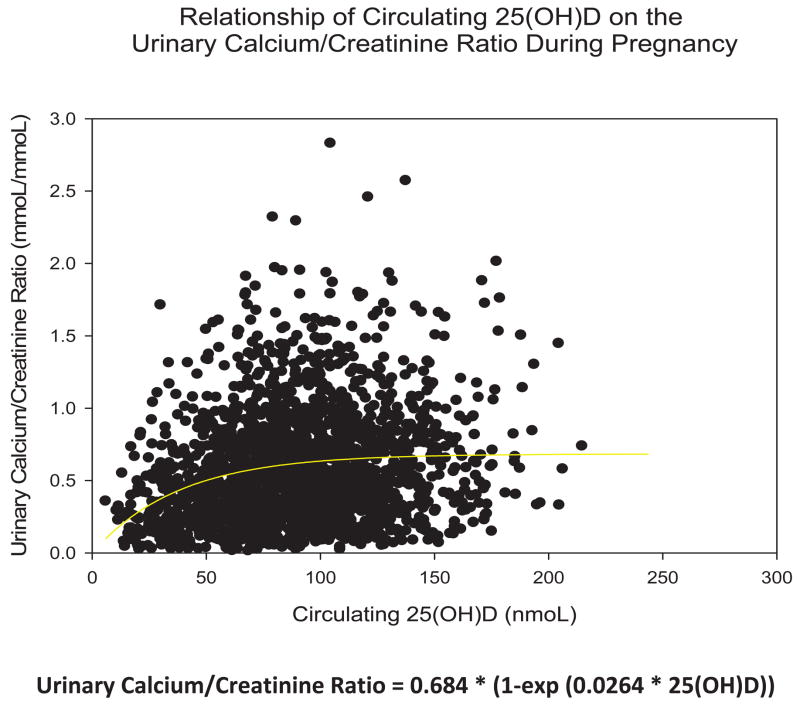
The need, safety, and effectiveness of vitamin D supplementation during pregnancy remain controversial. In this randomized, controlled trial, women with a singleton pregnancy at 12 to 16 weeks' gestation received 400, 2000, or 4000 IU of vitamin D(3) per day until delivery. The primary outcome was maternal/neonatal circulating 25-hydroxyvitamin D [25(OH)D] concentration at delivery, with secondary outcomes of a 25(OH)D concentration of 80 nmol/L or greater achieved and the 25(OH)D concentration required to achieve maximal 1,25-dihydroxyvitamin D(3) [1,25(OH)(2)D(3)] production. Of the 494 women enrolled, 350 women continued until delivery: Mean 25(OH)D concentrations by group at delivery and 1 month before delivery were significantly different (p < 0.0001), and the percent who achieved sufficiency was significantly different by group, greatest in 4000-IU group (p < 0.0001). The relative risk (RR) for achieving a concentration of 80 nmol/L or greater within 1 month of delivery was significantly different between the 2000- and the 400-IU groups (RR = 1.52, 95% CI 1.24-1.86), the 4000- and the 400-IU groups (RR = 1.60, 95% CI 1.32-1.95) but not between the 4000- and. 2000-IU groups (RR = 1.06, 95% CI 0.93-1.19). Circulating 25(OH)D had a direct influence on circulating 1,25(OH)(2)D(3) concentrations throughout pregnancy (p < 0.0001), with maximal production of 1,25(OH)(2)D(3) in all strata in the 4000-IU group. There were no differences between groups on any safety measure. Not a single adverse event was attributed to vitamin D supplementation or circulating 25(OH)D levels. It is concluded that vitamin D supplementation of 4000 IU/d for pregnant women is safe and most effective in achieving sufficiency in all women and their neonates regardless of race, whereas the current estimated average requirement is comparatively ineffective at achieving adequate circulating 25(OH)D concentrations, especially in African Americans.
Copyright © 2011 American Society for Bone and Mineral Research.
Conflict of interest statement
All other authors (DDJ, TCH, ME, and CLW) state that they have no conflicts of interests.
Figures
Comment in
-
Vitamin D supplementation during pregnancy.J Bone Miner Res. 2011 Oct;26(10):2338-40. doi: 10.1002/jbmr.498. J Bone Miner Res. 2011. PMID: 21948703 No abstract available.
References
-
- Hatun S, Ozkan B, Orbak Z, Doneray H, Cizmecioglu F, Toprak D, Calikoglu AS. Vitamin D Deficiency in Early Infancy. J Nutr. 2005;135(2):279–282. - PubMed
-
- Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122(5):1142–1152. - PubMed
-
- Yorifuji J, Yorifuji T, Tachibana K, Nagai S, Kawai M, Momoi T, Nagasaka H, Hatayama H, Nakahata T. Craniotabes in normal newborns: the earliest sign of subclinical vitamin D deficiency. J Clin Endocrinol Metab. 2008;93(5):1784–1788. - PubMed
-
- Anatoliotaki M, Tsilimigaki A, Tsekoura T, Schinaki A, Stefanaki S, Nicolaidou P. Congenital rickets due to maternal vitamin D deficiency in a sunny island of Greece. Acta Paediatr. 2003;92 (3):389–391. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
