

Phase II trial of cetuximab, gemcitabine, and oxaliplatin followed by chemoradiation with cetuximab for locally advanced (T4) pancreatic adenocarcinoma: correlation of Smad4(Dpc4) immunostaining with pattern of disease progression
- PMID: 21709185
- PMCID: PMC3157965
- DOI: 10.1200/JCO.2010.33.8038
Phase II trial of cetuximab, gemcitabine, and oxaliplatin followed by chemoradiation with cetuximab for locally advanced (T4) pancreatic adenocarcinoma: correlation of Smad4(Dpc4) immunostaining with pattern of disease progression
Abstract
Purpose: This phase II trial was designed to assess the efficacy and safety of cetuximab, gemcitabine, and oxaliplatin followed by cetuximab, capecitabine, and radiation therapy in locally advanced pancreatic cancer (LAPC).
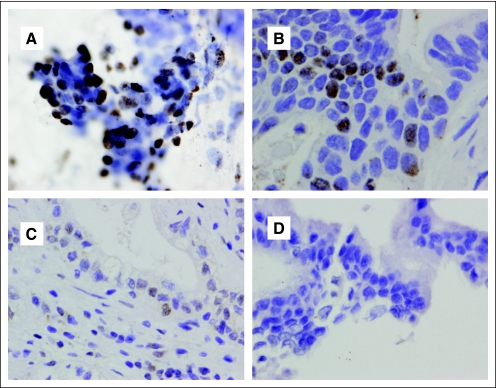
Patients and methods: Treatment-naive eligible patients (n = 69) received intravenous gemcitabine (1,000 mg/m(2)) and oxaliplatin (100 mg/m(2)) every 2 weeks for four doses, followed by radiation (50.4 Gy to the gross tumor only) with concurrent capecitabine (825 mg/m(2) twice daily on radiation treatment days). Cetuximab (500 mg/m(2)) was started on day 1 of chemotherapy and was continued every 2 weeks during chemotherapy and chemoradiotherapy. Diagnostic cytology specimens were immunostained for Smad4(Dpc4) expression.
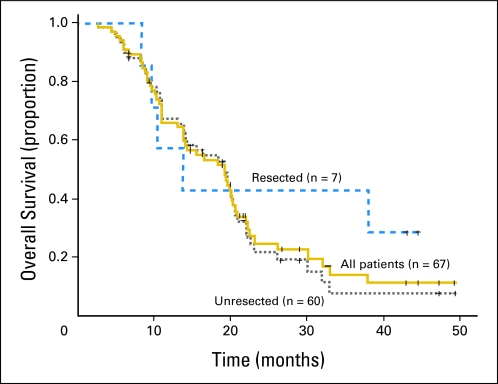
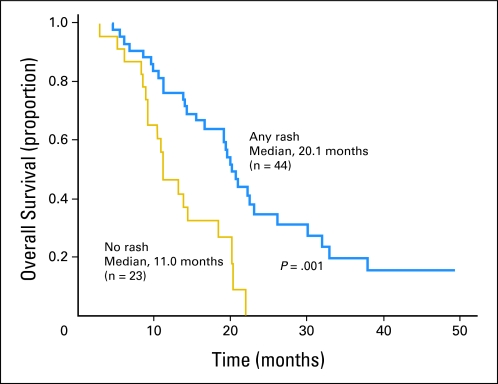
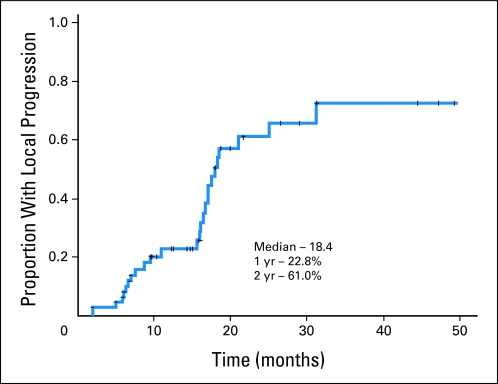
Results: Median overall survival time was 19.2 months (95% CI, 14.2 to 24.2 months), and 1-year, 2-year, and 4-year actuarial overall survival rates were 66.0%, 25.02%, and 11.3%, respectively. Acneiform rash correlated with improved survival (P = .001), but initial CA19-9, borderline resectable initial stage, and surgical resection (n = 7) did not. The 1-year and 2-year radiographic local progression rates were 22.8% and 61.0%, respectively. The worst acute toxic effects were GI toxicity (32% and 10% for grades 2 and 3, respectively); fatigue (26% and 6% for grades 2 and 3, respectively); sensory neuropathy (9% and 1% for grades 2 and 3, respectively); and acneiform rash (54% and 3% for grades 2 and 3, respectively). Smad4(Dpc4) expression correlated with a local rather than a distant dominant pattern of disease progression (P = .016).
Conclusion: This regimen appears effective and has acceptable toxicity. The primary end point (1-year overall survival rate > 45%) was met, with encouraging survival duration. Smad4(Dpc4) immunostaining correlated with the pattern of disease progression. Prospective validation of Smad4(Dpc4) expression in cytology specimens as a predictive biomarker is warranted and may lead to personalized treatment strategies for patients with localized pancreatic cancer.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Chauffert B, Mornex F, Bonnetain F, et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer: Definitive results of the 2000-2001 FFCD/SFRO study. Ann Oncol. 2008;19:1592–1599. - PubMed
-
- Loehrer P, Powell M, Cardenes H, et al. A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized, unresectable pancreatic cancer: E4201. J Clin Oncol. 2008;26(suppl):214s. abstr 4506. - PubMed
-
- Krishnan S, Rana V, Janjan NA, et al. Induction chemotherapy selects patients with locally advanced, unresectable pancreatic cancer for optimal benefit from consolidative chemoradiation therapy. Cancer. 2007;110:47–55. - PubMed
-
- Huguet F, André T, Hammel P, et al. Impact of chemoradiotherapy after disease control with chemotherapy in locally advanced pancreatic adenocarcinoma in GERCOR phase II and III studies. J Clin Oncol. 2007;25:326–331. - PubMed
-
- Xiong HQ, Rosenberg A, LoBuglio A, et al. Cetuximab, a monoclonal antibody targeting the epidermal growth factor receptor, in combination with gemcitabine for advanced pancreatic cancer: A multicenter phase II Trial. J Clin Oncol. 2004;22:2610–2616. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
