

Secondary somatic mutations restoring BRCA1/2 predict chemotherapy resistance in hereditary ovarian carcinomas
- PMID: 21709188
- PMCID: PMC3157963
- DOI: 10.1200/JCO.2010.34.2980
Secondary somatic mutations restoring BRCA1/2 predict chemotherapy resistance in hereditary ovarian carcinomas
Abstract
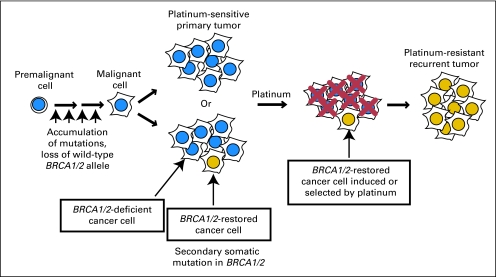
Purpose: Secondary somatic BRCA1/2 mutations may restore BRCA1/2 protein in hereditary ovarian carcinomas. In cell lines, BRCA2 restoration mediates resistance to platinum chemotherapy and poly (ADP-ribose) polymerase (PARP) inhibitors. We assessed primary and recurrent BRCA1/2-mutated ovarian carcinomas to define the frequency of secondary mutations and correlate these changes with clinical outcomes.
Methods: Neoplastic cells were isolated with laser capture microdissection, and DNA was sequenced at the site of the known germline BRCA1/2 mutation. When secondary mutations were found that restored wild-type sequence, haplotyping was performed using single nucleotide polymorphisms in tumor and paired lymphocyte DNA to rule out retention of the wild-type allele.
Results: There were 64 primary and 46 recurrent ovarian carcinomas assessed. Thirteen (28.3%) of 46 (95% CI, 17.3% to 42.6%) recurrent carcinomas had a secondary mutation compared with two (3.1%) of 64 (95% CI, 1.0% to 10.7%) primary carcinomas (P = .0003, Fisher's exact test). Twelve (46.2%) of 26 (95% CI, 28.7% to 64.7%) platinum-resistant recurrences had secondary mutations restoring BRCA1/2, compared with one (5.3%) of 19 (95% CI, 1.2% to 24.8%) platinum-sensitive recurrences (P = .003, Fisher's exact test). Six (66.7%) of nine (95% CI, 34.8% to 87.8%) women with prior breast carcinoma had a recurrent carcinoma with a secondary mutation, compared with six (17.1%) of 35 (95% CI, 8.2% to 32.8%) with no history of breast carcinoma (P = .007, Fisher's exact test).
Conclusion: Secondary somatic mutations that restore BRCA1/2 in carcinomas from women with germline BRCA1/2 mutations predict resistance to platinum chemotherapy and may also predict resistance to PARP inhibitors. These mutations were detectable only in ovarian carcinomas of women whom have had previous chemotherapy, either for ovarian or breast carcinoma.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures




Similar articles
-
BRCA mutation frequency and patterns of treatment response in BRCA mutation-positive women with ovarian cancer: a report from the Australian Ovarian Cancer Study Group.J Clin Oncol. 2012 Jul 20;30(21):2654-63. doi: 10.1200/JCO.2011.39.8545. Epub 2012 Jun 18. J Clin Oncol. 2012. PMID: 22711857 Free PMC article.
-
Diverse BRCA1 and BRCA2 Reversion Mutations in Circulating Cell-Free DNA of Therapy-Resistant Breast or Ovarian Cancer.Clin Cancer Res. 2017 Nov 1;23(21):6708-6720. doi: 10.1158/1078-0432.CCR-17-0544. Epub 2017 Aug 1. Clin Cancer Res. 2017. PMID: 28765325 Free PMC article.
-
Somatic mutations in BRCA1 and BRCA2 could expand the number of patients that benefit from poly (ADP ribose) polymerase inhibitors in ovarian cancer.J Clin Oncol. 2010 Aug 1;28(22):3570-6. doi: 10.1200/JCO.2009.27.2997. Epub 2010 Jul 6. J Clin Oncol. 2010. PMID: 20606085 Free PMC article.
-
Parp inhibitors as maintenance treatment in platinum sensitive recurrent ovarian cancer: An updated meta-analysis of randomized clinical trials according to BRCA mutational status.Cancer Treat Rev. 2019 Nov;80:101909. doi: 10.1016/j.ctrv.2019.101909. Epub 2019 Oct 9. Cancer Treat Rev. 2019. PMID: 31629204 Review.
-
PARP Inhibitors and the Evolving Landscape of Ovarian Cancer Management: A Review.BioDrugs. 2019 Jun;33(3):255-273. doi: 10.1007/s40259-019-00347-4. BioDrugs. 2019. PMID: 30895466 Review.
Cited by
-
Targeting Homologous Recombination Deficiency in Ovarian Cancer with PARP Inhibitors: Synthetic Lethal Strategies That Impact Overall Survival.Cancers (Basel). 2022 Sep 23;14(19):4621. doi: 10.3390/cancers14194621. Cancers (Basel). 2022. PMID: 36230543 Free PMC article. Review.
-
PARP Inhibitor Resistance Mechanisms and Implications for Post-Progression Combination Therapies.Cancers (Basel). 2020 Jul 25;12(8):2054. doi: 10.3390/cancers12082054. Cancers (Basel). 2020. PMID: 32722408 Free PMC article. Review.
-
NF-κB signaling mediates acquired resistance after PARP inhibition.Oncotarget. 2015 Feb 28;6(6):3825-39. doi: 10.18632/oncotarget.2868. Oncotarget. 2015. PMID: 25686825 Free PMC article.
-
Role of PARP inhibitors in cancer biology and therapy.Curr Med Chem. 2012;19(23):3907-21. doi: 10.2174/092986712802002464. Curr Med Chem. 2012. PMID: 22788767 Free PMC article. Review.
-
Rucaparib Monotherapy in Patients With Pancreatic Cancer and a Known Deleterious BRCA Mutation.JCO Precis Oncol. 2018;2018:PO.17.00316. doi: 10.1200/PO.17.00316. Epub 2018 May 16. JCO Precis Oncol. 2018. PMID: 30051098 Free PMC article.
References
-
- Pal T, Permuth-Wey J, Betts JA, et al. BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases. Cancer. 2005;104:2807–2816. - PubMed
-
- Moynahan ME, Chiu JW, Koller BH, et al. Brca1 controls homology-directed DNA repair. Mol Cell. 1999;4:511–518. - PubMed
-
- Moynahan ME, Pierce AJ, Jasin M. BRCA2 is required for homology-directed repair of chromosomal breaks. Mol Cell. 2001;7:263–272. - PubMed
-
- Neuhausen SL, Marshall CJ. Loss of heterozygosity in familial tumors from three BRCA1-linked kindreds. Cancer Res. 1994;54:6069–6072. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
