

Randomized phase II trials: a long-term investment with promising returns
- PMID: 21709274
- PMCID: PMC3139588
- DOI: 10.1093/jnci/djr218
Randomized phase II trials: a long-term investment with promising returns
Abstract
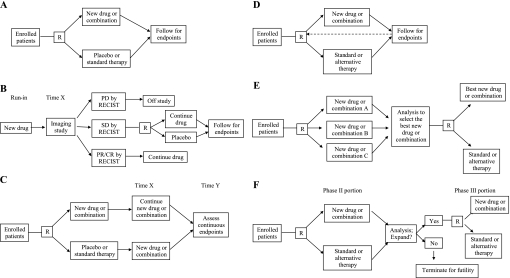
Given the multitude of novel anticancer drugs and the limited resources available to study them, phase II trials should identify drugs with the highest probability of succeeding in subsequent phase III trials. Currently, single-arm phase II trial results are interpreted relative to historical control subjects, introducing selection bias and confounding that may limit the validity of the conclusions. The rate of success (defined as a statistically significant difference between arms) in phase III oncology trials is only 40%, suggesting that current phase II trials are insufficiently informative. However, simulation studies suggest that randomized phase II trials would have lower error rates and greater predictive power for phase III results. Randomized phase II trials may also be more informative than single-arm phase II trials because of the hypotheses being tested, the variety of possible endpoints, and the opportunities for biomarker discovery. There are a wide variety of randomized phase II designs that can be used, including the randomized discontinuation design, the delayed-start design, adaptive (Bayesian) designs, selection designs, and phase II/III designs. The barriers to widespread adoption of randomized phase II trials include time to completion, sample size considerations, and ethical concerns, but none are insurmountable. We conclude that randomized phase II trials are a worthy investment considering finite patient and financial resources and should be the rule rather than the exception for evaluating novel therapies in oncology.
Figures
Comment in
-
More randomization in phase II trials: necessary but not sufficient.J Natl Cancer Inst. 2011 Jul 20;103(14):1075-7. doi: 10.1093/jnci/djr238. Epub 2011 Jun 27. J Natl Cancer Inst. 2011. PMID: 21709273 Free PMC article. No abstract available.
References
-
- Adams CP, Brantner VV. Estimating the cost of new drug development: is it really 802 million dollars? Health Aff (Millwood). 2006;25(2):420–428. - PubMed
-
- Kola I, Landis J. Can the pharmaceutical industry reduce attrition rates? Nat Rev Drug Discov. 2004;3(8):711–715. - PubMed
-
- Elias T, Gordian M, Singh N, et al. Why products fail in phase III. In Vivo. 2006;24:49–54.
-
- Michaelis LC, Ratain MJ. Phase II trials published in 2002: a cross-specialty comparison showing significant design differences between oncology trials and other medical specialties. Clin Cancer Res. 2007;13(8):2400–2405. - PubMed
