

Presentation, diagnosis, pathophysiology, and treatment of the neurological features of Sturge-Weber syndrome
- PMID: 21712663
- PMCID: PMC4487915
- DOI: 10.1097/NRL.0b013e318220c5b6
Presentation, diagnosis, pathophysiology, and treatment of the neurological features of Sturge-Weber syndrome
Abstract
Background: Sturge-Weber syndrome (SWS) is a neurovascular disorder with a capillary malformation of the face (port-wine birthmark), a capillary-venous malformation in the eye, and a capillary-venous malformation in the brain (leptomeningeal angioma). Although SWS is a congenital disorder usually presenting in infancy, occasionally neurological symptoms first present in adulthood and most affected individuals do survive into adulthood with varying degrees of neurological impairment including epilepsy, hemiparesis, visual field deficits, and cognitive impairments ranging from mild learning disabilities to severe deficits. SWS is a multisystem disorder that requires the neurologist to be aware of the possible endocrine, psychiatric, ophthalmologic, and other medical issues that can arise and impact the neurological status of these patients. Some of these clinical features have only recently been described.
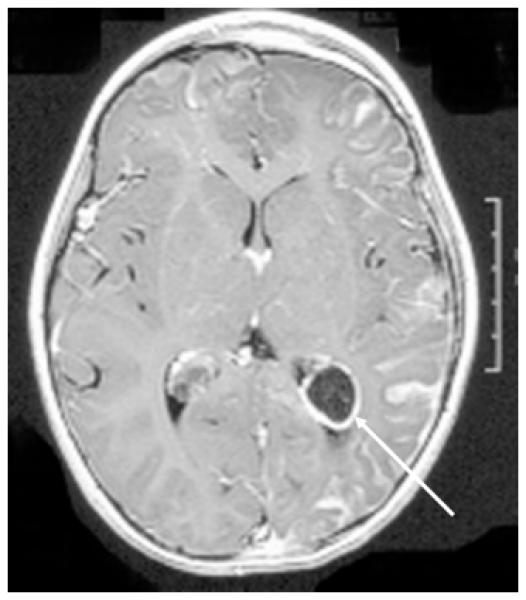
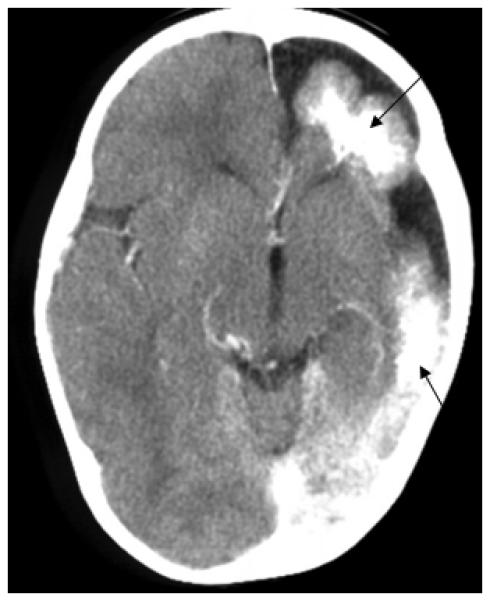
Review summary: This review summarizes the neurological manifestations of SWS, discusses issues related to the diagnosis of brain involvement, relates major neuroimaging findings, briefly describes the current understanding of pathogenesis, and provides an overview of neurological treatment strategies.
Conclusions: Recent clinical research has highlighted several novel and lesser-known aspects of this clinical syndrome including endocrine disorders. Functional imaging studies and clinical experience suggests that neurological progression results primarily from impaired blood flow and that prolonged seizures may contribute to this process. Treatment is largely symptomatic although aggressive efforts to prevent seizures and strokes, in young children especially, may impact outcome.
Figures
References
-
- Bodensteiner John B., Roach ES. Sturge-Weber syndrome: Introduction and Overview. John B.Bodensteiner and E.S.Roach; 1999. pp. 1–10.
-
- Ewen JB, Comi AM, Kossoff EH. Myoclonic-astatic epilepsy in a child with sturge-weber syndrome. Pediatr Neurol. 2007;36:115–117. - PubMed
-
- Kossoff EH, Ferenc L, Comi AM. An infantile-onset, severe, yet sporadic seizure pattern is common in Sturge-Weber syndrome. Epilepsia. 2009;50:2154–2157. - PubMed
-
- Fukuyama Y, Tsuchiya S. A study on Sturge-Weber syndrome. Report of a case associated with infantile spasms and electroencephalographic evolution in five cases. Eur Neurol. 1979;18:194–204. - PubMed
-
- Maria BL, Neufeld JA, Rosainz LC, et al. Central nervous system structure and function in Sturge-Weber syndrome: evidence of neurologic and radiologic progression. J Child Neurol. 1998;13:606–618. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
