

The diagnosis and treatment of autoimmune blistering skin diseases
- PMID: 21712975
- PMCID: PMC3123771
- DOI: 10.3238/arztebl.2011.0399
The diagnosis and treatment of autoimmune blistering skin diseases
Abstract
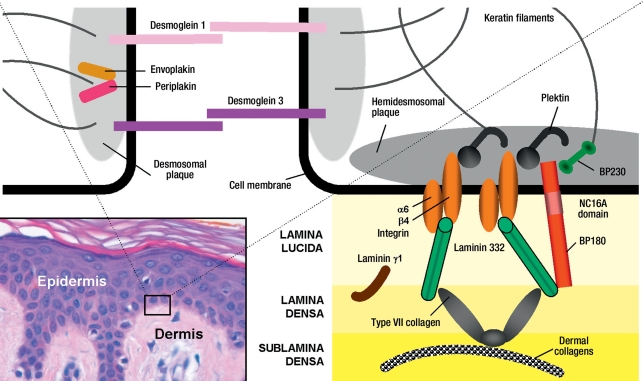
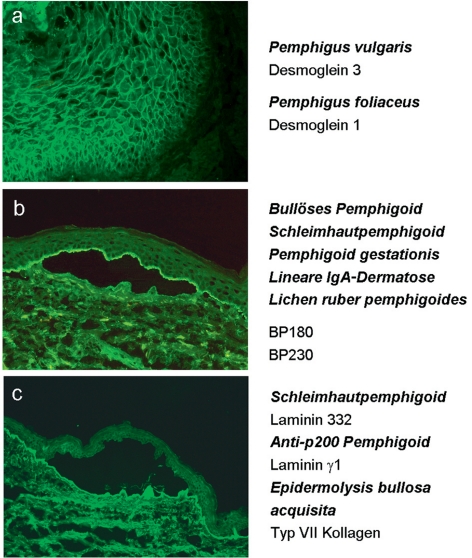
Background: Autoimmune blistering skin diseases are a heterogeneous group of disorders associated with autoantibodies that are directed against desmosomal structural proteins (in pemphigus diseases) or hemidesmosomal ones (in pemphigoid diseases and epidermolysis bullosa acquisita), or else against epidermal/ tissue transglutaminases (in dermatitis herpetiformis). Knowledge of the clinical presentation of these disorders and of the relevant diagnostic procedures is important not just for dermatologists, but also for general practitioners, ophthalmologists, ENT specialists, dentists, gynecologists, and pediatricians.
Methods: The literature on the subject was selectively reviewed. There are no existing guidelines available in Germany.
Results: The recently developed sensitive and specific assays for circulating autoantibodies in these diseases now enable a serological diagnosis in about 90% of cases. The incidence of autoimmune blistering skin diseases in Germany has doubled in the last 10 years, to a current figure of about 25 new cases per million persons per year, because of improved diagnostic techniques as well as the aging of the population. Accurate and specific diagnosis is the prerequisite for reliable prognostication and appropriate treatment. For severe and intractable cases, more effective treatments have recently become available, including immunoadsorption, high-dose intravenous immunoglobulin, the anti-CD20 antibody rituximab, and combinations of the above.
Conclusion: The diagnostic assessment of autoimmune blistering skin diseases can be expected to improve in the near future as new serological testing systems are developed that employ recombinant forms of the target antigens. The treatments currently in use still need to be validated by prospective, controlled trials.
Figures

References
-
- Schmidt E, Dähnrich C, Rosemann A, et al. Novel ELISA systems for antibodies to desmoglein 1 and 3. Correlation of disease activity with serum autoantibody levels in individual pemphigus patients. 2010;19:458–463. - PubMed
-
- Egan CA, Lazarova Z, Darling TN, Yee C, Cote T, Yancey KB. Anti-epiligrin cicatricial pemphigoid and relative risk for cancer. Lancet. 2001;357:1850–1851. - PubMed
-
- Zillikens D, Kawahara Y, Ishiko A, et al. A novel subepidermal blistering disease with autoantibodies to a 200-kDa antigen of the basement membrane zone. J Invest Dermatol. 1996;106:1333–1338. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous