

The influence of reduced susceptibility to fluoroquinolones in Salmonella enterica serovar Typhi on the clinical response to ofloxacin therapy
- PMID: 21713025
- PMCID: PMC3119645
- DOI: 10.1371/journal.pntd.0001163
The influence of reduced susceptibility to fluoroquinolones in Salmonella enterica serovar Typhi on the clinical response to ofloxacin therapy
Abstract
Background: Infection with Salmonella enterica serovar Typhi (S. Typhi) with reduced susceptibility to fluoroquinolones has been associated with fluoroquinolone treatment failure. We studied the relationship between ofloxacin treatment response and the ofloxacin minimum inhibitory concentration (MIC) of the infecting isolate. Individual patient data from seven randomised controlled trials of antimicrobial treatment in enteric fever conducted in Vietnam in which ofloxacin was used in at least one of the treatment arms was studied. Data from 540 patients randomised to ofloxacin treatment was analysed to identify an MIC of the infecting organism associated with treatment failure.
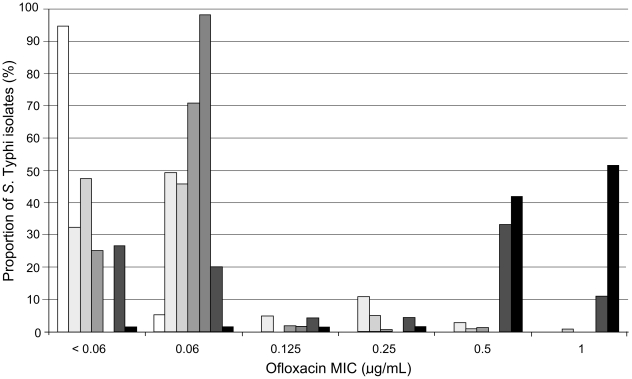
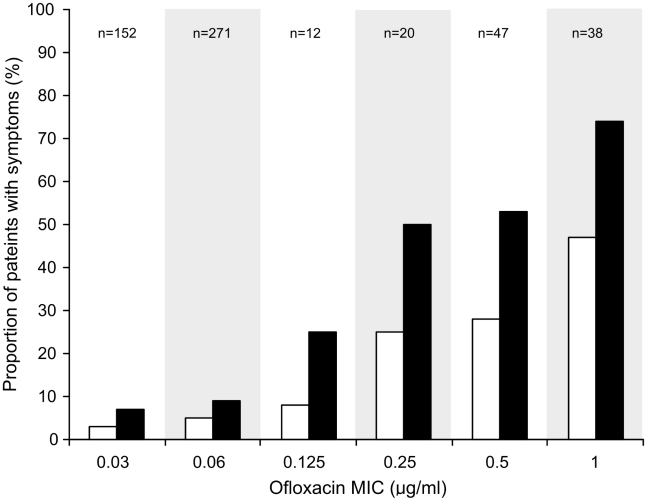
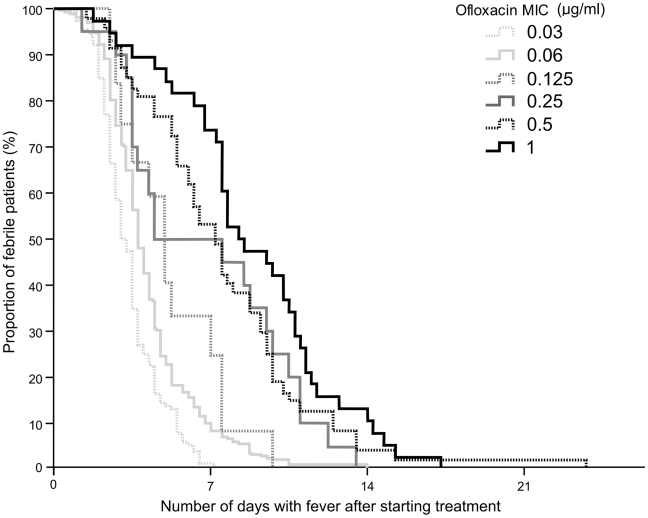
Principal findings: The proportion of patients failing ofloxacin treatment was significantly higher in patients infected with S. Typhi isolates with an MIC≥0.25 µg/mL compared with those infections with an MIC of ≤0.125 µg/mL (p<0.001). Treatment success was 96% when the ofloxacin MIC was ≤0.125 µg/mL, 73% when the MIC was between 0.25 and 0.50 µg/mL and 53% when the MIC was 1.00 µg/mL. This was despite a longer duration of treatment at a higher dosage in patients infected with isolates with an MIC≥0.25 µg/mL compared with those infections with an MIC of ≤0.125 µg/mL.
Significance: There is a clear relationship between ofloxacin susceptibility and clinical outcome in ofloxacin treated patients with enteric fever. An ofloxacin MIC of ≥0.25 µg/mL, or the presence of nalidixic acid resistance, can be used to define S. Typhi infections in which the response to ofloxacin may be impaired.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Parry CM, Threlfall EJ. Antimicrobial resistance in typhoidal and nontyphoidal salmonellae. Curr Opin Infect Dis. 2008;21:531–538. - PubMed
-
- WHO. The diagnosis, treatment and prevention of typhoid fever. Communicable Disease Surveillance and Response Vaccine and Biologicals. 2003:7–18. ( http://whqlibdoc.who.int/hq/2003/WHO_V&B_2003.2007.pdf)
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
