

High-dose fenoldopam reduces postoperative neutrophil gelatinase-associated lipocaline and cystatin C levels in pediatric cardiac surgery
- PMID: 21714857
- PMCID: PMC3219034
- DOI: 10.1186/cc10295
High-dose fenoldopam reduces postoperative neutrophil gelatinase-associated lipocaline and cystatin C levels in pediatric cardiac surgery
Abstract
Introduction: The aim of the study was to evaluate the effects of high-dose fenoldopam, a selective dopamine-1 receptor, on renal function and organ perfusion during cardiopulmonary bypass (CPB) in infants with congenital heart disease (CHD).
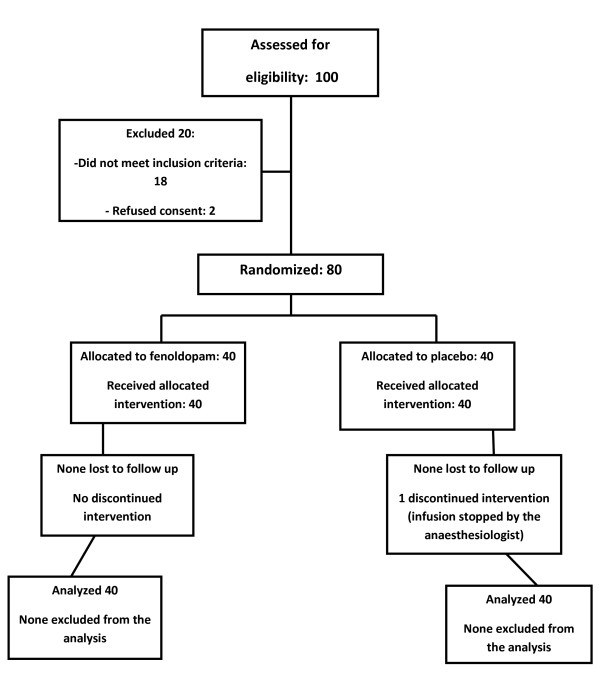
Methods: A prospective single-center randomized double-blind controlled trial was conducted in a pediatric cardiac surgery department. We randomized infants younger than 1 year with CHD and biventricular anatomy (with exclusion of isolated ventricular and atrial septal defect) to receive blindly a continuous infusion of fenoldopam at 1 μg/kg/min or placebo during CPB. Perioperative urinary and plasma levels of neutrophil gelatinase-associated lipocaline (NGAL), cystatin C (CysC), and creatinine were measured to assess renal injury after CPB.
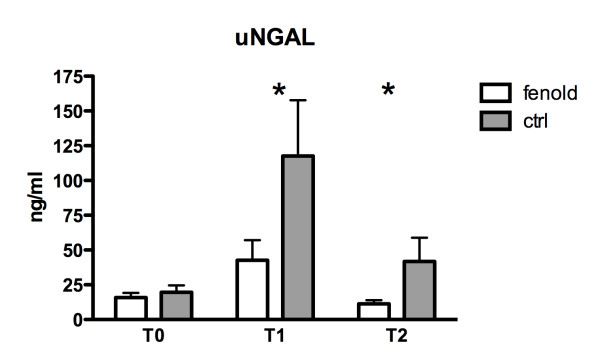
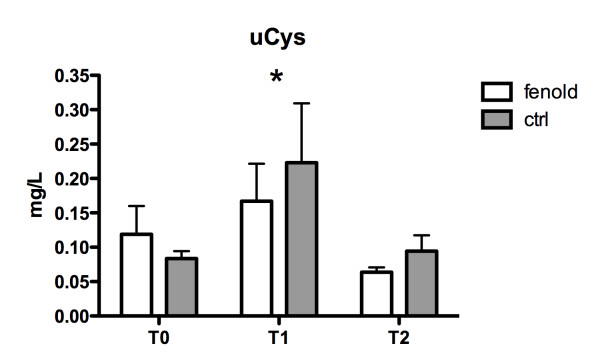
Results: We enrolled 80 patients: 40 received fenoldopam (group F) during CPB, and 40 received placebo (group P). A significant increase of urinary NGAL and CysC levels from baseline to intensive care unit (ICU) admission followed by restoration of normal values after 12 hours was observed in both groups. However, urinary NGAL and CysC values were significantly reduced at the end of surgery and 12 hours after ICU admission (uNGAL only) in group F compared with group P (P = 0.025 and 0.039, respectively). Plasma NGAL and CysC tended to increase from baseline to ICU admission in both groups, but they were not significantly different between the two groups. No differences were observed on urinary and plasma creatinine levels and on urine output between the two groups. Acute kidney injury (AKI) incidence in the postoperative period, as indicated by pRIFLE classification (pediatric score indicating Risk, Injury, Failure, Loss of function, and End-stage kidney disease level of renal damage) was 50% in group F and 72% in group P (P = 0.08; odds ratio (OR), 0.38; 95% confidence interval (CI), 0.14 to 1.02). A significant reduction in diuretics (furosemide) and vasodilators (phentolamine) administration was observed in group F (P = 0.0085; OR, 0.22; 95% CI, 0.07 to 0.7).
Conclusions: The treatment with high-dose fenoldopam during CPB in pediatric patients undergoing cardiac surgery for CHD with biventricular anatomy significantly decreased urinary levels of NGAL and CysC and reduced the use of diuretics and vasodilators during CPB.
Trial registration: Clinical Trial.Gov NCT00982527.
Figures
Comment in
-
A novel use for novel acute kidney injury biomarkers: fenoldopam's effect on neutrophil gelatinase-associated lipocalin and cystatin C.Crit Care. 2011 Aug 2;15(4):177. doi: 10.1186/cc10296. Crit Care. 2011. PMID: 21861863 Free PMC article.
References
-
- Chiravuri SD, Riegger LQ, Christensen R, Butler RR, Malviya S, Tait AR, Voepel-Lewis T. Factors associated with acute kidney injury or failure in children undergoing cardiopulmonary bypass: a case-controlled study. Paediatr Anaesth. 2011;21:880–886. doi: 10.1111/j.1460-9592.2011.03532.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
