

Reduction of thyroid nodule volume by levothyroxine and iodine alone and in combination: a randomized, placebo-controlled trial
- PMID: 21715542
- PMCID: PMC3206705
- DOI: 10.1210/jc.2011-0356
Reduction of thyroid nodule volume by levothyroxine and iodine alone and in combination: a randomized, placebo-controlled trial
Abstract
Context: Nodular goiter is common worldwide, but there is still debate over the medical treatment.
Objective: The objective of the study was the measurement of the effect of a treatment with (nonsuppressive) T(4), iodine, or a combination of both compared with placebo on volume of thyroid nodules and thyroid.
Design: This was a multicenter, randomized, double-blind trial in patients with nodular goiter in Germany [LISA (Levothyroxin und Iodid in der Strumatherapie Als Mono-oder Kombinationstherapie) trial].
Setting: The study was conducted in outpatient clinics in university hospitals and regional hospitals and private practices.
Participants: One thousand twenty-four consecutively screened and centrally randomized euthyroid patients aged 18-65 yr with one or more thyroid nodules (minimal diameter 10 mm) participated in the study.
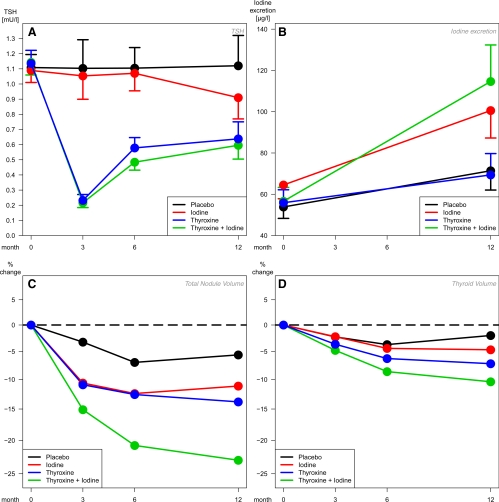
Intervention: Intervention included placebo, iodine (I), T(4), or T(4)+I for 1 yr. T(4) doses were adapted for a TSH target range of 0.2-0.8 mU/liter.
Outcome measures: The primary end point was percent volume reduction of all nodules measured by ultrasound, and the main secondary end point was a change in goiter volume.
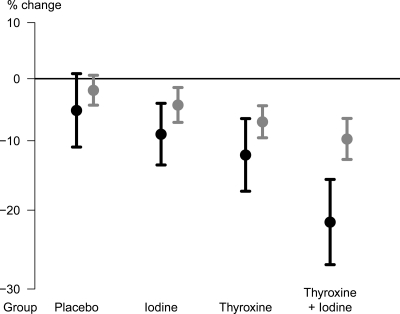
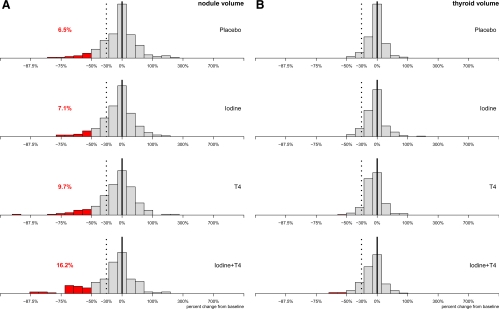
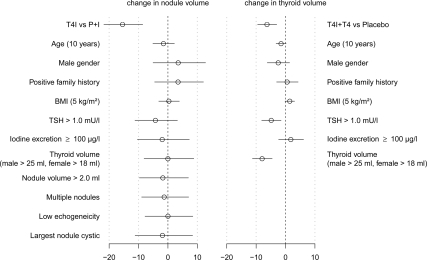
Results: Nodule volume reductions were -17.3% [95% confidence interval (CI) -24.8/-9.0%, P < 0.001] in the T(4)+I group, -7.3% (95% CI -15.0/+1.2%, P = 0.201) in the T(4) group, and -4.0% (95% CI -11.4/+4.2%, P = 0.328) in the I group as compared with placebo. In direct comparison, the T(4)+I therapy was significantly superior to T(4) (P = 0.018) or I (P = 0.003). Thyroid volume reductions were -7.9% (95% CI -11.8/-3.9%, P < 0.001), -5.2% (95% CI -8.7/-1.6%, P = 0.024) and -2.5% (95% CI -6.2/+1.4%, P = 0.207), respectively. The T(4)+I therapy was significantly superior to I (P = 0.034) but not to T(4) (P = 0.190).
Conclusion: In a region with a sufficient iodine supply, a 1-yr therapy with a combination of I and T(4) with incomplete suppression of thyrotropin reduced thyroid nodule volume further than either component alone or placebo.
Figures
References
-
- Völzke H, Lüdemann J, Robinson DM, Spieker KW, Schwahn C, Kramer A, John U, Meng W. 2003. The prevalence of undiagnosed thyroid disorders in a previously iodine-deficient area. Thyroid 13:803–810 - PubMed
-
- Knudsen N, Bülow I, Jorgensen T, Laurberg P, Ovesen L, Perrild H. 2000. Goitre prevalence and thyroid abnormalities at ultrasonography: a comparative epidemiological study in two regions with slightly different iodine status. Clin Endocrinol (Oxf) 53:479–485 - PubMed
-
- Laurberg P, Jørgensen T, Perrild H, Ovesen L, Knudsen N, Pedersen IB, Rasmussen LB, Carlé A, Vejbjerg P. 2006. The Danish investigation on iodine intake and thyroid disease, DanThyr: status and perspectives. Eur J Endocrinol 155:219–228 - PubMed
-
- Brander A, Viikinkoski P, Nickels J, Kivisaari L. 1989. Thyroid gland: US screening in middle-aged women with no previous thyroid disease. Radiology 173:507–510 - PubMed
-
- Bruneton JN, Balu-Maestro C, Marcy PY, Melia P, Mourou MY. 1994. Very high frequency (13 MHz) ultrasonographic examination of the normal neck: detection of normal lymph nodes and thyroid nodules. J Ultrasound Med 13:87–90 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
