

The cost-effectiveness of symptom-based testing and routine screening for acute HIV infection in men who have sex with men in the USA
- PMID: 21716076
- PMCID: PMC3657607
- DOI: 10.1097/QAD.0b013e328349f067
The cost-effectiveness of symptom-based testing and routine screening for acute HIV infection in men who have sex with men in the USA
Abstract
Objective: Acute HIV infection often causes influenza-like illness (ILI) and is associated with high infectivity. We estimated the effectiveness and cost-effectiveness of strategies to identify and treat acute HIV infection in men who have sex with men (MSM) in the USA.
Design: Dynamic model of HIV transmission and progression.
Interventions: We evaluated three testing approaches: viral load testing for individuals with ILI, expanded screening with antibody testing, and expanded screening with antibody and viral load testing. We included treatment with antiretroviral therapy for individuals identified as acutely infected.
Main outcome measures: New HIV infections, discounted quality-adjusted life years (QALYs) and costs, and incremental cost-effectiveness ratios.
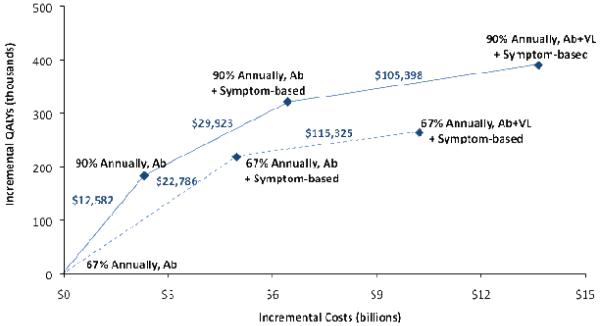
Results: At the present rate of HIV-antibody testing, we estimated that 538,000 new infections will occur among MSM over the next 20 years. Expanding antibody screening coverage to 90% of MSM annually reduces new infections by 2.8% and costs US$ 12,582 per QALY gained. Symptom-based viral load testing with ILI is more expensive than expanded antibody screening, but is more effective and costs US$ 22,786 per QALY gained. Combining expanded antibody screening with symptom-based viral load testing prevents twice as many infections compared to expanded antibody screening alone, and costs US$ 29,923 per QALY gained. Adding viral load testing to all annual HIV tests costs more than US$ 100,000 per QALY gained.
Conclusion: Use of HIV viral load testing in MSM with ILI prevents more infections than does expanded annual antibody screening alone and is inexpensive relative to other screening interventions. Clinicians should consider symptom-based viral load testing in MSM, in addition to encouraging annual antibody screening.
Figures
References
-
- Centers for Disease Control and Prevention (CDC) [Accessed September 30, 2009];Estimates of New HIV Infections in the United States. 2008 http://www.cdc.gov/hiv/topics/surveillance/resources/factsheets/incidenc....
-
- Centers for Disease Control and Prevention (CDC) [Accessed September 30, 2009];HIV Prevalence Estimates -- United States, 2006. 2008 http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5739a2.htm.
-
- Centers for Disease Control and Prevention (CDC) [Accessed January 27, 2010];HIV/AIDS Surveillance Special Report, Number 5 - HIV Testing Survey, 2002. 2006 http://www.cdc.gov/hiv/topics/surveillance/resources/reports/2004spec_no....
-
- Centers for Disease Control and Prevention (CDC) Human immunodeficiency virus (HIV) risk, prevention, and testing behaviors -- United States, National HIV Behavioral Surveillance System: Men who have sex with men, November 2003-April 2005. MMWR Morbid Mortal Wkly Rep. 2006;55:1–16. - PubMed
-
- Centers for Disease Control and Prevention (CDC) Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55:1–17. quiz CE11-14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
