

Objective assessment of utility of intraoperative ultrasound in resection of central nervous system tumors: A cost-effective tool for intraoperative navigation in neurosurgery
- PMID: 21716843
- PMCID: PMC3123010
- DOI: 10.4103/0976-3147.80077
Objective assessment of utility of intraoperative ultrasound in resection of central nervous system tumors: A cost-effective tool for intraoperative navigation in neurosurgery
Abstract
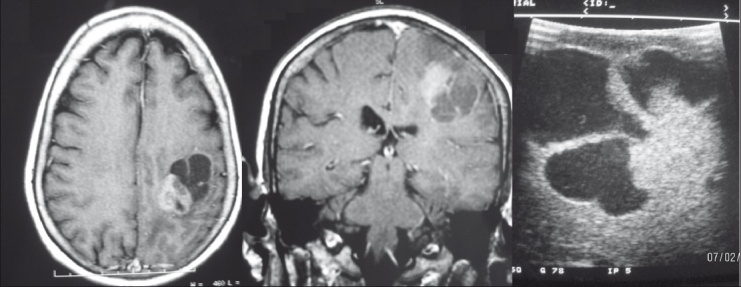
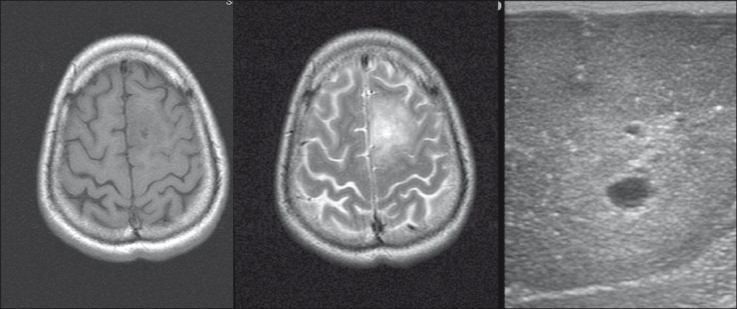
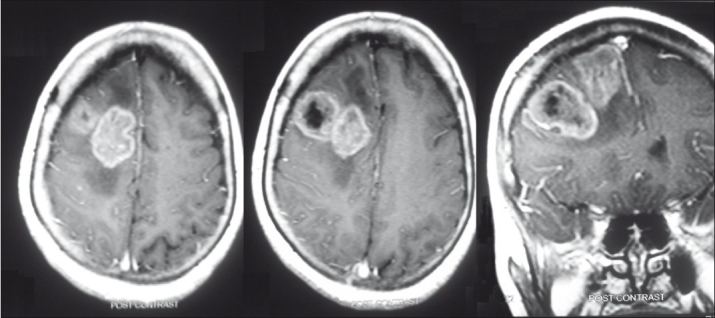
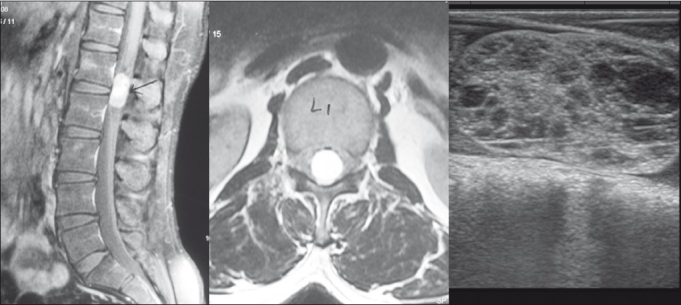
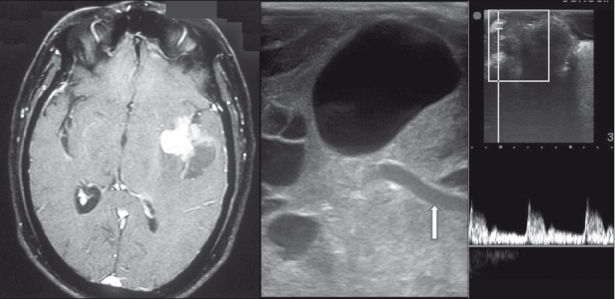
Background: Localization and delineation of extent of lesions is critical for safe maximal resection of brain and spinal cord tumors. Frame-based and frameless stereotaxy and intraoperative MRI are costly and not freely available especially in economically constrained nations. Intraoperative ultrasound has been around for a while but has been relegated to the background. Lack of objective evidence for its usefulness and the perceived "user unfriendliness" of US are probably responsible for this. We recount our experience with this "forgotten" tool and propose an objective assessment score of its utility in an attempt to revive this practice.
Materials and methods: Seventy seven intraoperative ultrasound (IOUS) studies were carried out in patients with brain and spinal cord tumors. Seven parameters were identified to measure the "utility" of the IOUS and a "utility score" was devised (minimum 0 and maximum 7). Individual parameter and overall scores were calculated for each case.
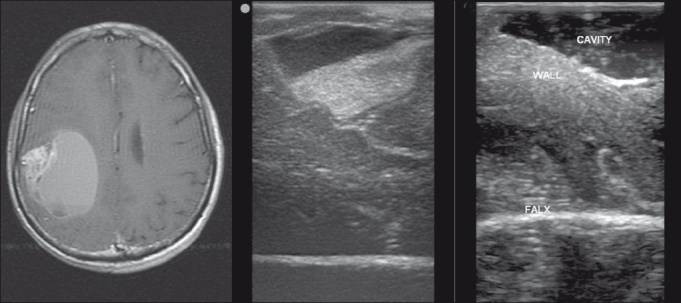
Results: IOUS was found to be useful in many ways. The median overall score was 6 (mean score 5.65). There were no scores less than 4 with the majority demonstrating usefulness in 5 or more parameters (91%). The use of the IOUS significantly influenced the performance of the surgery in these cases without significantly prolonging surgery.
Conclusions: The IOUS is a very useful tool in intraoperative localization and delineation of lesions and planning various stages of tumor resection. It is easy, convenient, reliable, widely available, and above all a cost-effective tool. It should be increasingly used by neurosurgeons in the developing world where costlier intraoperative localization and imaging is not available freely.
Keywords: Cost-effective; intraoperative imaging; intraoperative ultrasound; scoring system; utility.
Conflict of interest statement
Figures
References
-
- Yaşargil MG, Kadri PA, Yasargil DC. Microsurgery for malignant gliomas. J Neurooncol. 2004;69:67–81. - PubMed
-
- Pia HW. Microsurgery of gliomas. Acta Neurochir (Wien) 1986;80:1–11. - PubMed
-
- Dohrmann GJ, Rubin JM. History of intraoperative ultrasound in neurosurgery. Neurosurg Clin N Am. 2001;12:155–66. - PubMed
-
- Rubin JM, Mirfakhraee M, Duda EE, Dohrmann GJ, Brown F. Intraoperative ultrasound examination of the brain. Radiology. 1980;137:831–2. - PubMed
-
- Rubin JM, Dohrmann GJ, Chandler WF. Intraoperative spinal ultrasonography. Clin Neurosurg. 1988;34:282–312. - PubMed
LinkOut - more resources
Full Text Sources