

Spinal shortening and monosegmental posterior spondylodesis in the management of dorsal and lumbar unstable injuries
- PMID: 21716869
- PMCID: PMC3122988
- DOI: 10.4103/0976-3147.80082
Spinal shortening and monosegmental posterior spondylodesis in the management of dorsal and lumbar unstable injuries
Abstract
Introduction: Patients with spinal injuries have been treated in the past by laminectomy in an attempt to decompress the spinal cord. The results have shown insignificant improvement or even a worsening of neurologic function and decreased stability without effectively removing the anterior bone and disc fragments compressing the spinal cord. The primary indication for anterior decompression and grafting is narrowing of the spinal canal with neurologic deficits that cannot be resolved by any other approach. One must think of subsequent surgical intervention for increased stability and compressive posterior fusion with short-armed internal fixators.
Aim: To analyze the results and efficacy of spinal shortening combined with interbody fusion technique for the management of dorsal and lumbar unstable injuries.
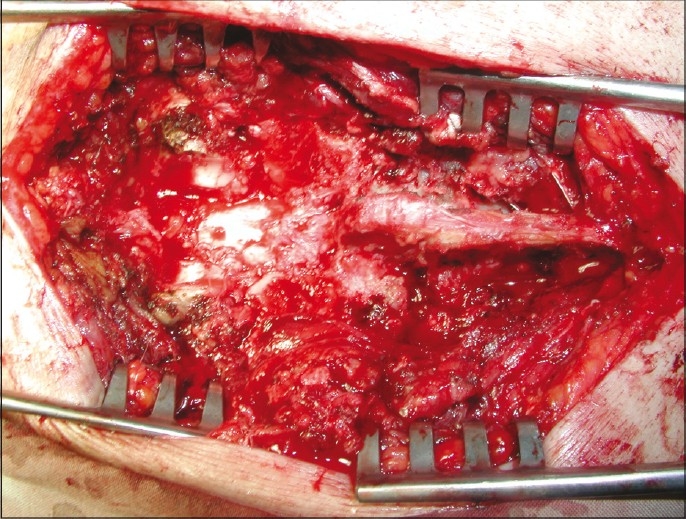
Materials and methods: Twenty-three patients with traumatic fractures and or fracture-dislocation of dorsolumbar spine with neurologic deficit are presented. All had radiologic evidence of spinal cord or cauda equina compression, with either paraplegia or paraparesis. Patients underwent recapping laminoplasty in the thoracic or lumbar spine for decompression of spinal cord. The T-saw was used for division of the posterior elements. After decompression of the cord and removal of the extruded bone fragments and disc material, the excised laminae were replaced exactly in situ to their original anatomic position. Then application of a compression force via monosegmental transpedicular fixation was done, allowing vertebral end-plate compression and interbody fusion.
Results: Lateral Cobb angle (T(10)-L(2)) was reduced from 26 to 4 degrees after surgery. The shortened vertebral body united and no or minimal loss of correction was seen. The preoperative vertebral kyphosis averaged +17 degrees and was corrected to +7 degrees at follow-up with the sagittal index improving from 0.59 to 0.86. The segmental local kyphosis was reduced from +15 degrees to -3 degrees. Radiography demonstrated anatomically correct reconstruction in all patients, as well as solid fusion.
Conclusion: This technique permits circumferential decompression of the spinal cord through a posterior approach and posterior interbody fusion.
Keywords: Injury; laminoplasty; shortening; spine; spondylodesis.
Conflict of interest statement
Figures





References
-
- Fehlings MG, Tator CH. An evidence-based review of decompressive surgery in acute spinal cord injury: Rational, indications, and timing based on experimental and clinical studies. J Neurosurgery (Spine 1) 1999;91:1–11. - PubMed
-
- Been HD, Bouma GJ. Comparison of two types of surgery for thoraco- lumbar burst fractures: Combined anterior and posterior stabilization vs.posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349–57. - PubMed
-
- Muhlbauer M, Pfisterer W, Eyb R, Knosp Minimally invasive retroperitoneal approach for lumbar corpectomy and anterior reconstruction.Technical note. J Neurosurg. 2000;93:161–7. - PubMed
-
- Saita K, Hoshino Y, Kikkawa I, Nakamura H. Posterior spinal shortening for paraplegia after vertebral collapse caused by osteoporosis. Spine. 2000;25:2832–5. - PubMed
-
- Schnee CL, Ansell LV. Selection criteria and outcome of operative approaches for thoracolumbar burst fractures with and without neurological deficit. J Neurosurg. 1997;86:48–55. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous