

Underascertainment of radiotherapy receipt in Surveillance, Epidemiology, and End Results registry data
- PMID: 21717446
- PMCID: PMC3224683
- DOI: 10.1002/cncr.26295
Underascertainment of radiotherapy receipt in Surveillance, Epidemiology, and End Results registry data
Abstract
Background: Surveillance, Epidemiology, and End Results (SEER) registry data have been used to suggest underuse and disparities in receipt of radiotherapy. Prior studies have cautioned that SEER may underascertain radiotherapy but lacked adequate representation to assess whether underascertainment varies by geography or patient sociodemographic characteristics. The authors sought to determine rates and correlates of underascertainment of radiotherapy in recent SEER data.
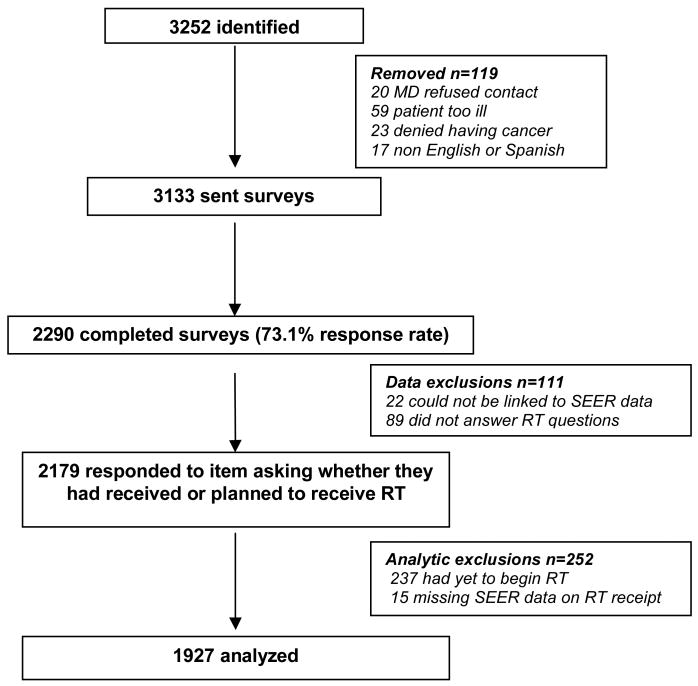
Methods: The authors evaluated data from 2290 survey respondents with nonmetastatic breast cancer, aged 20 to 79 years, diagnosed from June of 2005 to February 2007 in Detroit and Los Angeles and reported to SEER registries (73% response rate). Survey responses regarding treatment and sociodemographic factors were merged with SEER data. The authors compared radiotherapy receipt as reported by patients versus SEER records. The authors then assessed correlates of radiotherapy underascertainment in SEER.
Results: Of 1292 patients who reported receiving radiotherapy, 273 were coded as not receiving radiotherapy in SEER (underascertained). Underascertainment was more common in Los Angeles than in Detroit (32.0% vs 11.25%, P < .001). On multivariate analysis, radiotherapy underascertainment was significantly associated in each registry (Los Angeles, Detroit) with stage (P = .008, P = .026), income (P < .001, P = .050), mastectomy receipt (P < .001, P < .001), chemotherapy receipt (P < .001, P = .045), and diagnosis at a hospital that was not accredited by the American College of Surgeons (P < .001, P < .001). In Los Angeles, additional significant variables included younger age (P < .001), nonprivate insurance (P < .001), and delayed receipt of radiotherapy (P < .001).
Conclusions: SEER registry data as currently collected may not be an appropriate source for documentation of rates of radiotherapy receipt or investigation of geographic variation in the radiation treatment of breast cancer.
Copyright © 2011 American Cancer Society.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
References
-
- National Cancer Institute. Surveillance Epidemiology and End Results. About SEER. Accessed online at http://seer.cancer.gov/about/ on 07/30/2010.
-
- Yu JB, Gross CP, Wilson LD, Smith BD. NCI SEER public-use data: applications and limitations in oncology research. Oncology. 2009;23(3):288–95. - PubMed
-
- Farrow DC, Hunt WC, Samet JM. Geographic variation in the treatment of localized breast cancer. NEJM. 1992;326(17):1097–101. - PubMed
-
- Nattinger AB, Hoffman RG, Kneusel RT, Schapira MM. Relation between appropriateness of primary therapy for early-stage breast carcinoma and increased use of breast-conserving surgery. The Lancet. 2000;356:1148–53. - PubMed
-
- SEER Program Coding and Staging Manual 2010. [Accessed online on 2/11/11]; at http://seer.cancer.gov/manuals/2010/SPCSM_2010_maindoc.pdf.
